
Gastrointestinal Surgery — MCQs

On this page
A wide mouth Meckel's diverticulum is found incidentally during laparotomy. What is the recommended treatment?
Paralytic ileus is characterized by which of the following findings, except?
Which of the following features characterize acute intestinal obstruction?
A 50-year-old woman presented with bilateral solid ovarian tumors, ascites, and an ulcerative growth in the pyloric region of the stomach. What is the most likely diagnosis?
What is the treatment of choice for perforation of the cervical esophagus?
A 60-year-old male is diagnosed with carcinoma of the stomach. A CT scan of the abdomen reveals a 4x4 cm mass in the antrum with involvement of celiac and right gastric nodes. What is the management of choice?
Which of the following statements is NOT true regarding gastrointestinal tuberculosis?
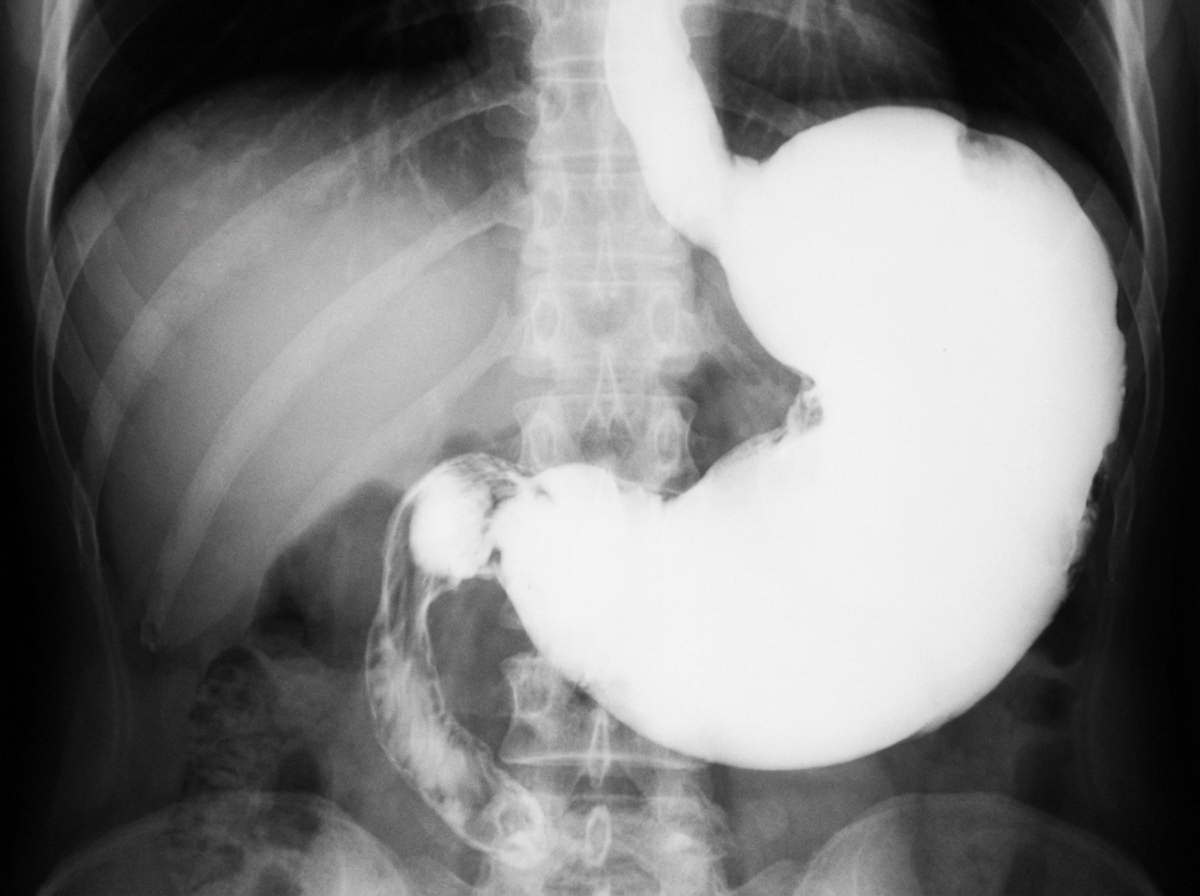
In an adult patient in a region with high gastric cancer prevalence, which is the most common cause of the below condition?
Which of the following is not an indication for splenectomy?
A patient with a gastric ulcer has a biopsy that reveals malignancy. What is the next step in management?
Practice by Chapter
Esophageal Disorders
Practice Questions
Gastric Disorders
Practice Questions
Small Intestine Pathology
Practice Questions
Appendicitis
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Diverticular Disease
Practice Questions
Anorectal Disorders
Practice Questions
Colorectal Neoplasms
Practice Questions
Gastrointestinal Stomas
Practice Questions
Bariatric Surgery Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app