
Gastrointestinal Surgery — MCQs

On this page
Which type of hernia is least likely to strangulate?
A 61-year-old female presents with a history of recurrent chest infections, regurgitation of food, and a feeling of fullness. What is the most probable diagnosis?
What is the standard treatment for squamous anal carcinoma?
Ileal resection is done for an adult patient developing intussusception due to which of the following causes?
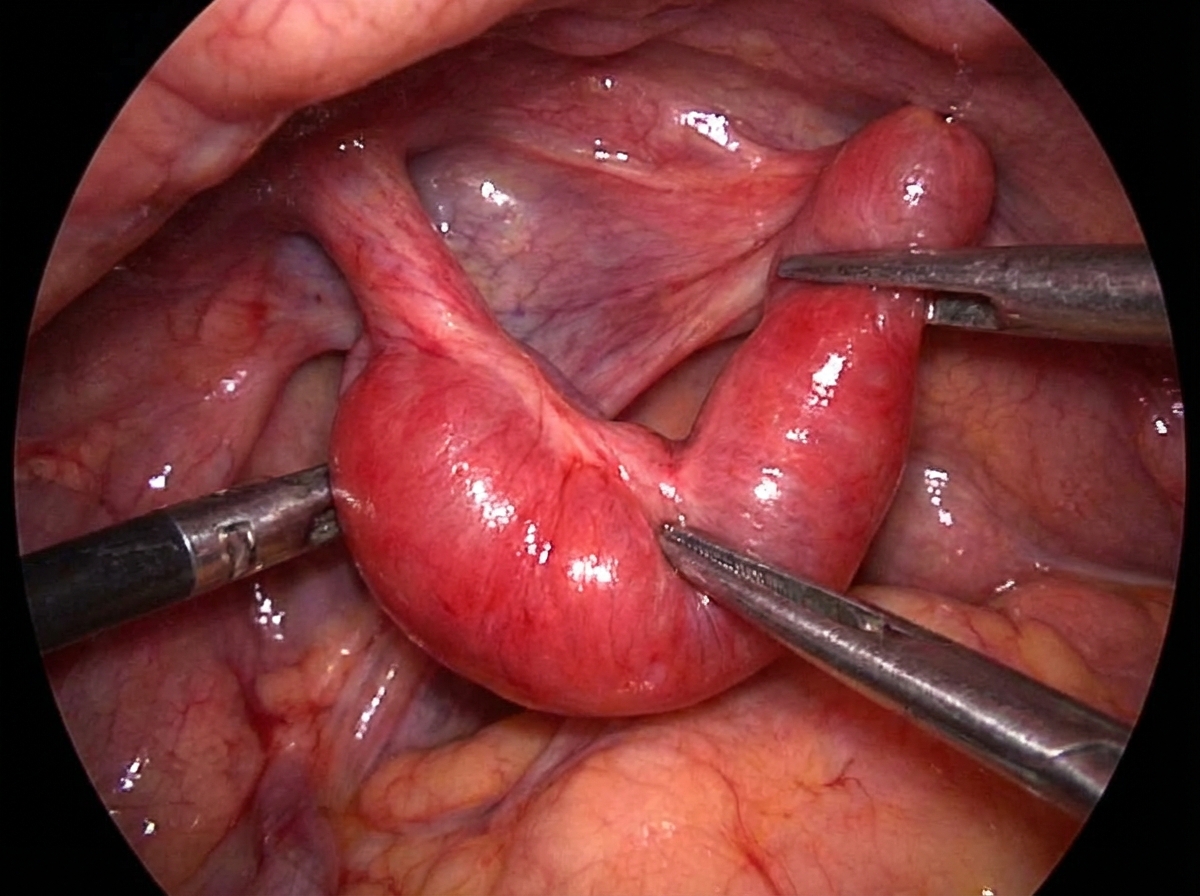
Which scoring system is used to diagnose the condition suggested by the surgical procedure shown in this adult patient?
What is the diagnostic method for early-stage carcinoma of the esophagus?
What is true about sliding esophageal hernia in all cases?
Mowat-Finke operation is done for which carcinoma?
Which of the following statements is not true about Meckel's diverticulum?
A 35-year-old CEO underwent an antrectomy and vagotomy for a bleeding ulcer. Although usually careful with his diet, he ate a large meal during a business lunch. Within 1 hour, he felt lightheaded and developed abdominal cramping and diarrhea. His symptoms may be attributed to:
Practice by Chapter
Esophageal Disorders
Practice Questions
Gastric Disorders
Practice Questions
Small Intestine Pathology
Practice Questions
Appendicitis
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Diverticular Disease
Practice Questions
Anorectal Disorders
Practice Questions
Colorectal Neoplasms
Practice Questions
Gastrointestinal Stomas
Practice Questions
Bariatric Surgery Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app