
Gastrointestinal Surgery — MCQs

On this page
Which of the following statements about hernia is false?
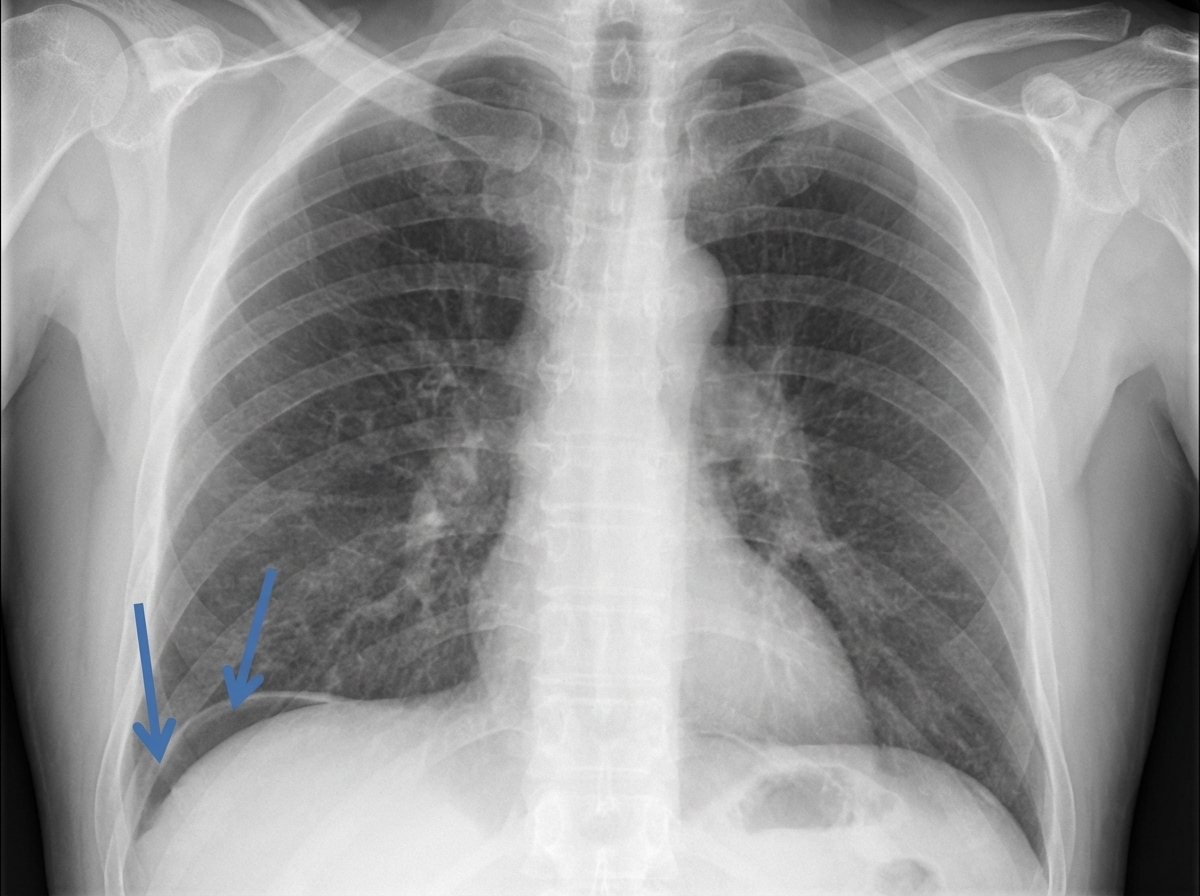
A patient presented to the emergency department with severe abdominal pain. An erect radiograph was performed. Based on the findings, what should be the management?
Which blood group is associated with gastric cancer?
What are the commonest sites of intra-abdominal abscess?
Which of the following are predisposing factors for Esophageal Carcinoma?
Which is the best method for supplementing nutrition in patients who have undergone massive resection of the small intestine?
A 58-year-old lady is diagnosed with carcinoma of the stomach. A CT scan of the abdomen shows a 4 cm mass in the antrum with involvement of the serosa. What is the treatment?
A female patient presents with dysphagia and intermittent epigastric pain. Endoscopy reveals esophageal dilatation above and narrowing at the lower end. What is the recommended treatment?
Which of the following investigations is useful in the evaluation of upper gastrointestinal bleeding?
A 23-year-old lady presents with acute right lower abdominal pain for the past 4 hours. There is tenderness at McBurney's point. Which investigation is best suited to confirm the diagnosis of appendicitis?
Practice by Chapter
Esophageal Disorders
Practice Questions
Gastric Disorders
Practice Questions
Small Intestine Pathology
Practice Questions
Appendicitis
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Diverticular Disease
Practice Questions
Anorectal Disorders
Practice Questions
Colorectal Neoplasms
Practice Questions
Gastrointestinal Stomas
Practice Questions
Bariatric Surgery Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app