
Gastrointestinal Surgery — MCQs

On this page
A patient presents with progressive dysphagia and a barium swallow shows a bird-beak appearance. What is the investigation of choice?
What is the most common site for carcinoma of the stomach?
Amyl nitrate inhalation test is used to detect which of the following conditions?
What is the most common symptom of bronchial adenoma?
Which of the following is NOT true about gastric carcinoma?
An elderly patient presented with early satiety and weight loss, attributing these symptoms to aging. Upper endoscopy revealed a large mass in the stomach. Which statement is TRUE regarding gastric carcinoma?
Which of the following is NOT a risk factor for carcinoma of the stomach?
Which statement is true regarding esophageal leiomyoma?
What is the investigation of choice for esophageal stricture caused by corrosive poisoning?
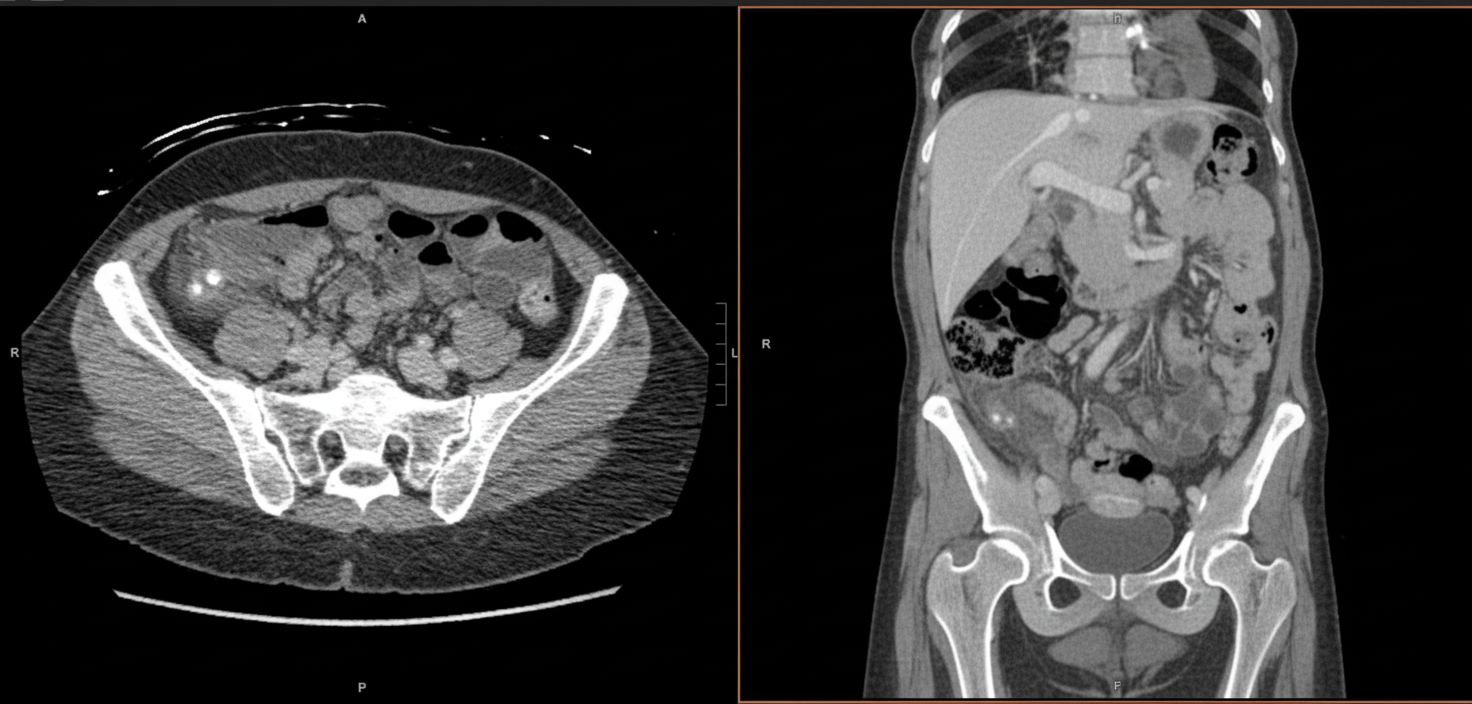
A 27-year-old woman presents with high fever and abdominal pain. Initially, the pain is around the navel but shifts to the right lower quadrant. A CT scan is provided. Which structure is affected?
Practice by Chapter
Esophageal Disorders
Practice Questions
Gastric Disorders
Practice Questions
Small Intestine Pathology
Practice Questions
Appendicitis
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Diverticular Disease
Practice Questions
Anorectal Disorders
Practice Questions
Colorectal Neoplasms
Practice Questions
Gastrointestinal Stomas
Practice Questions
Bariatric Surgery Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app