
Gastrointestinal Surgery — MCQs

On this page
Which dye is used in chromoendoscopy for the detection of cancer?
All of the following statements regarding the repair of groin hernias are true EXCEPT?
What is the most common cause of peritonitis in adult males?
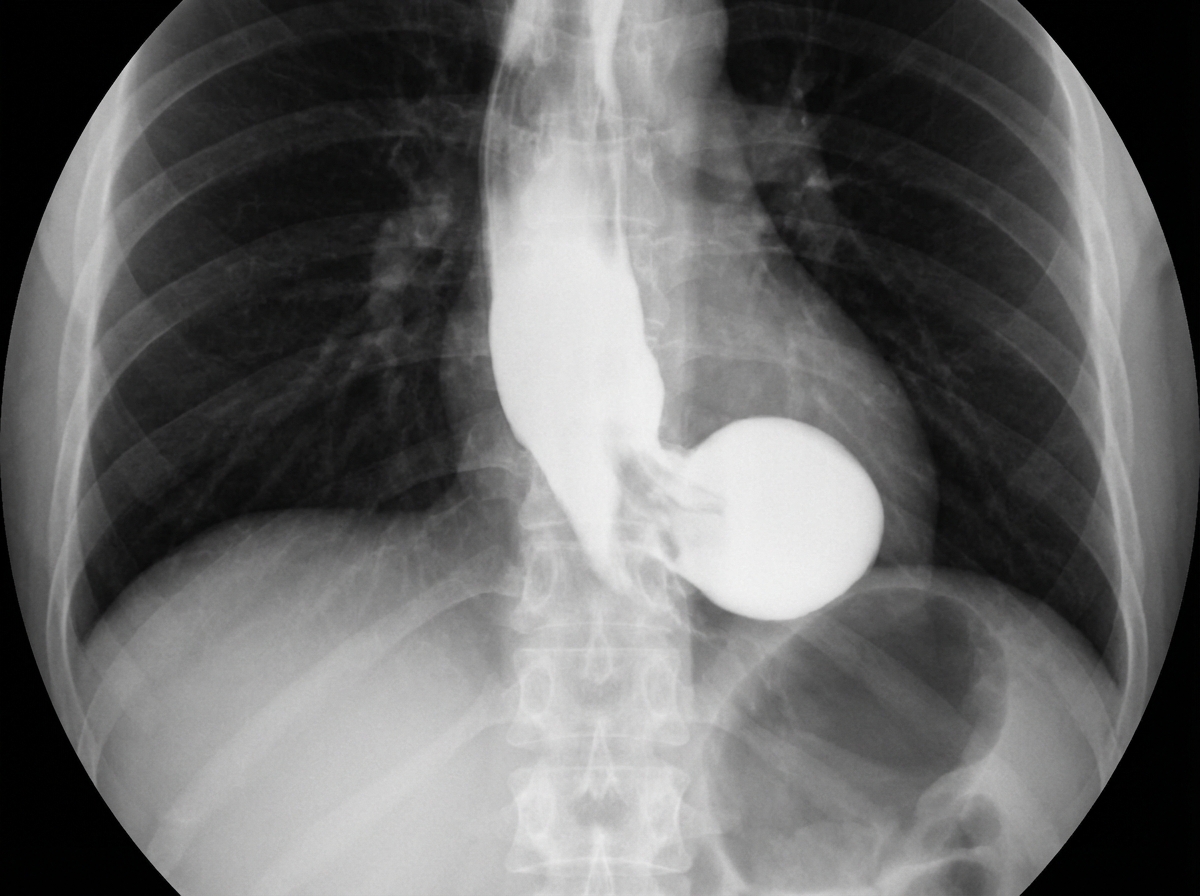
A 65-year-old patient presents with dysphagia and regurgitation. Barium swallow imaging is provided. What is the diagnosis?
Richter's hernia can be seen in all hernias except:
Cattle's maneuver is mobilization of:
Which of the following statements about Zenker's diverticulum is TRUE?
A 50-year-old male presented with progressive dysphagia for 4 months to solids, significant weight loss, loss of appetite, odynophagia, a hoarse voice, and cervical lymphadenopathy. Upper GI endoscopy with biopsy was performed. Which of the following barium findings would most likely correspond with this condition?
Which of the following statements is NOT true regarding Curling's ulcer?
What is the management for a strangulated hernia?
Practice by Chapter
Esophageal Disorders
Practice Questions
Gastric Disorders
Practice Questions
Small Intestine Pathology
Practice Questions
Appendicitis
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Diverticular Disease
Practice Questions
Anorectal Disorders
Practice Questions
Colorectal Neoplasms
Practice Questions
Gastrointestinal Stomas
Practice Questions
Bariatric Surgery Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app