
Gastrointestinal Surgery — MCQs

On this page
Which of the following is appropriate in the management of dumping syndrome?
An elderly man presented with sigmoid volvulus, which was successfully detorsed. What is the next definitive management step?
What is the most common type of hernia?
Which neoadjuvant chemotherapy is used in esophageal cancer?
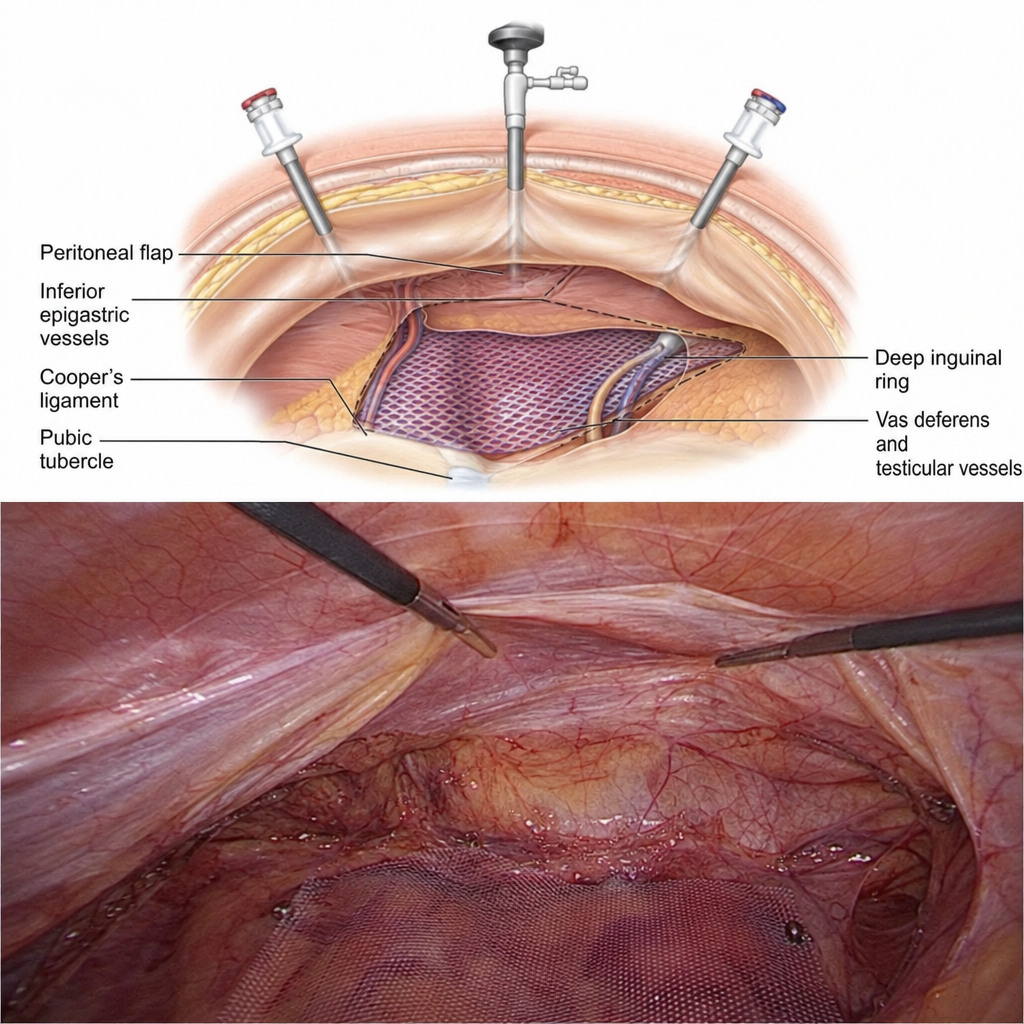
What is the name of the hernia repair technique depicted?
Sister Mary Joseph nodule suggests?
What is the most common site of carcinoma of the stomach?
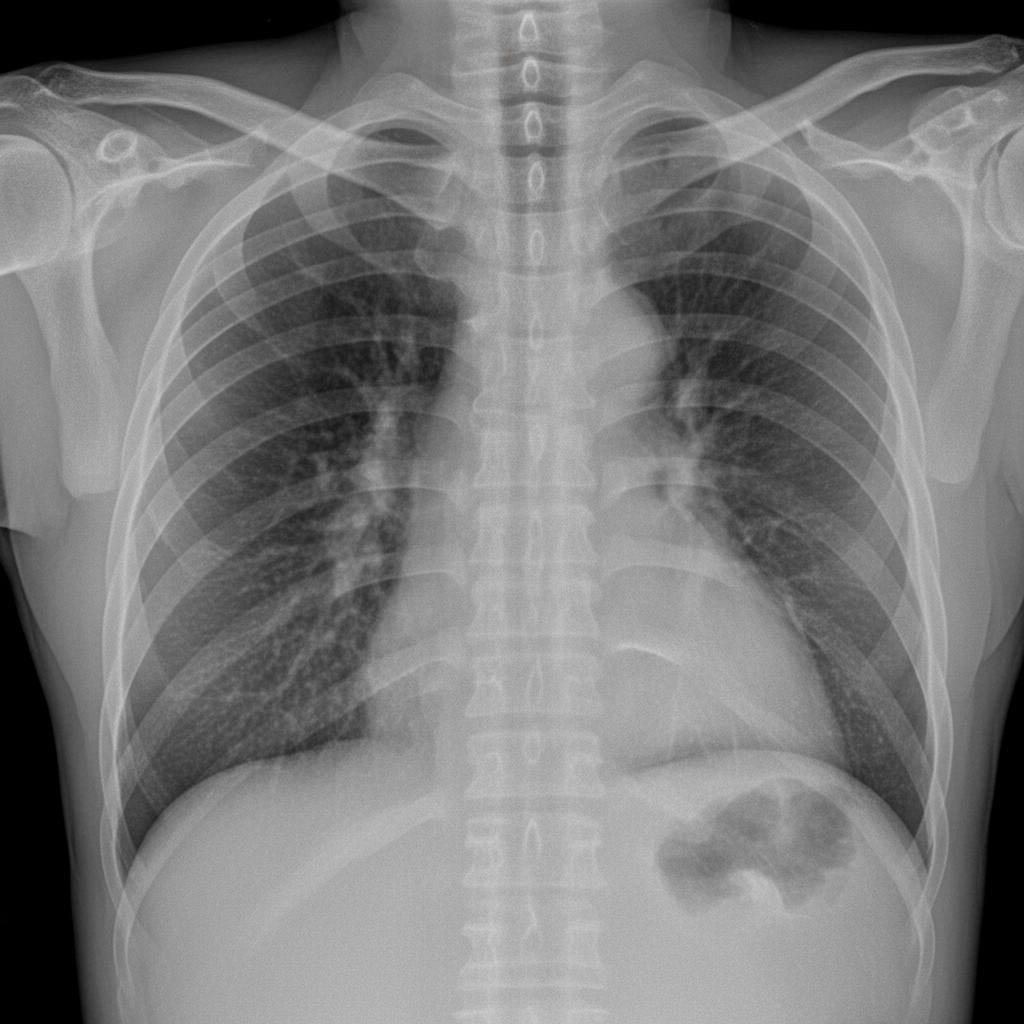
A 45-year-old male with a history of chronic duodenal ulcer presented to the emergency department in a state of shock. After resuscitation, investigations were performed. An erect chest X-ray demonstrating pneumoperitoneum (free air under the diaphragm) is provided. What is the preferred treatment option?
Which of the following is false regarding Barrett's esophagus?
A 36-year-old man presents with right scrotal swelling that began shortly after moving furniture. He denies nausea, vomiting, change in bowel habits, abdominal pain, or urinary tract symptoms. On examination, an enlarged right hemi-scrotum is noted, with a mass originating at the level of the external inguinal ring. The mass is reducible through the external inguinal ring. When the mass is reduced and the patient performs a Valsalva maneuver, a protrusion is felt at the external inguinal ring. The testicle appears normal after reduction. Which of the following pathological processes might cause the patient's underlying condition to occur in an infant?
Practice by Chapter
Esophageal Disorders
Practice Questions
Gastric Disorders
Practice Questions
Small Intestine Pathology
Practice Questions
Appendicitis
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Diverticular Disease
Practice Questions
Anorectal Disorders
Practice Questions
Colorectal Neoplasms
Practice Questions
Gastrointestinal Stomas
Practice Questions
Bariatric Surgery Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app