
Gastrointestinal Surgery — MCQs

On this page
Which is the commonest post-splenectomy infection?
A 35-year-old male with a six-year history of chronic duodenal ulcer presents with worsening of symptoms, loss of periodicity, pain on rising in the morning, a sense of epigastric bloating, and post-prandial vomiting. What is the most likely cause of the worsening of his symptoms?
Which of the following is NOT a predisposing factor for esophageal cancer?
Anemia is greater following which type of gastric resection?
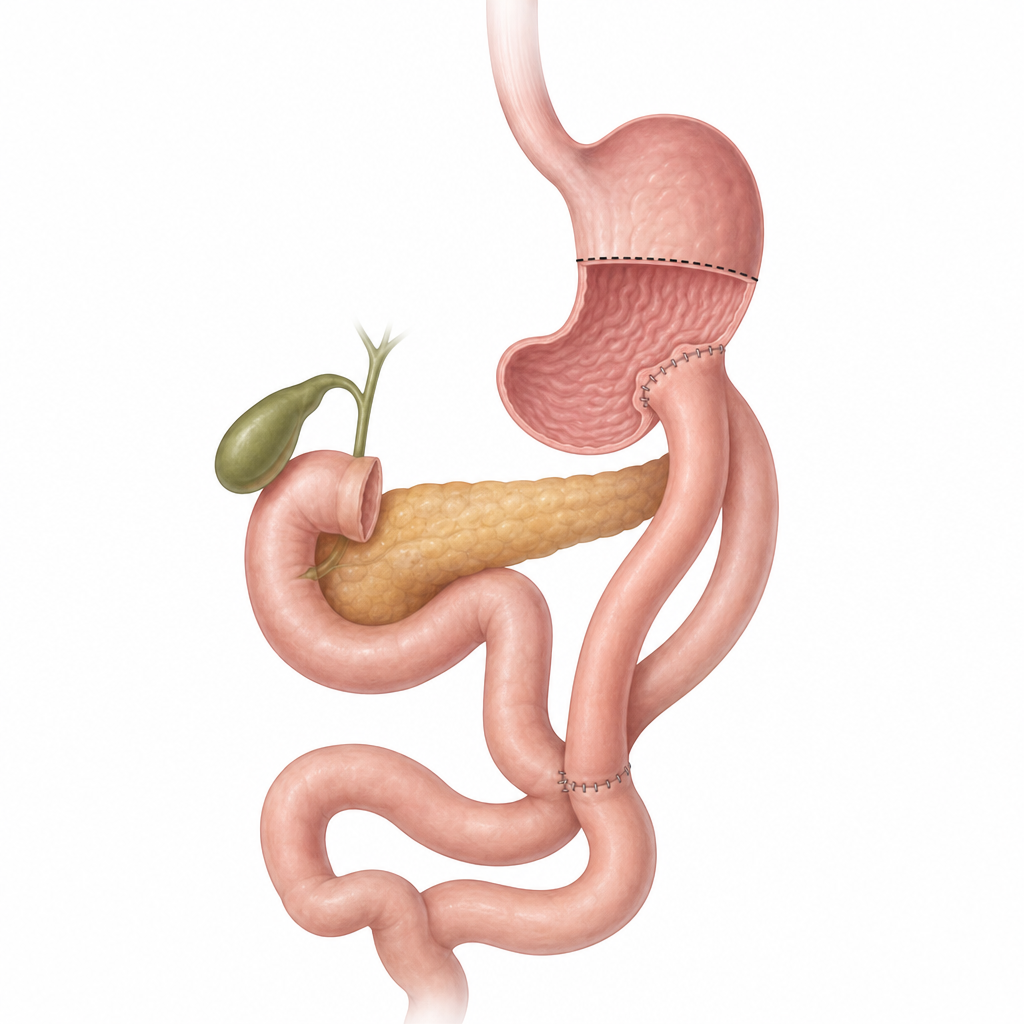
A patient with distal gastric carcinoma underwent a procedure. Name the procedure performed.
Early dumping syndrome is primarily due to which of the following mechanisms?
What is the most common presenting symptom of carcinoma of the stomach?
Which Borrmann class describes a linitis plastica?
While performing a radical gastrectomy for a 2 x 2 cm antral adenocarcinoma, which of the following structures is NOT typically removed?
A 70-year-old man presents with a 16-week history of progressive dysphagia and recurrent pneumonia episodes. He also has palpable stony hard neck nodes on examination. What is the most likely diagnosis?
Practice by Chapter
Esophageal Disorders
Practice Questions
Gastric Disorders
Practice Questions
Small Intestine Pathology
Practice Questions
Appendicitis
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Diverticular Disease
Practice Questions
Anorectal Disorders
Practice Questions
Colorectal Neoplasms
Practice Questions
Gastrointestinal Stomas
Practice Questions
Bariatric Surgery Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app