
Gastrointestinal Surgery — MCQs

On this page
Dysphagia lusoria is caused by which of the following?
Curling's ulcer is commonly found in which part of the duodenum?
According to the Nyhus classification, what type is a direct inguinal hernia?
The Rossetti modification of Nissen's fundoplication involves which of the following?
Laparoscopic operation for gastrointestinal reflux should be considered in a patient with any of the following situations, EXCEPT:
Which of the following is the best method to determine the depth of invasion in esophageal carcinoma?
Which of the following is FALSE about paraduodenal hernia?
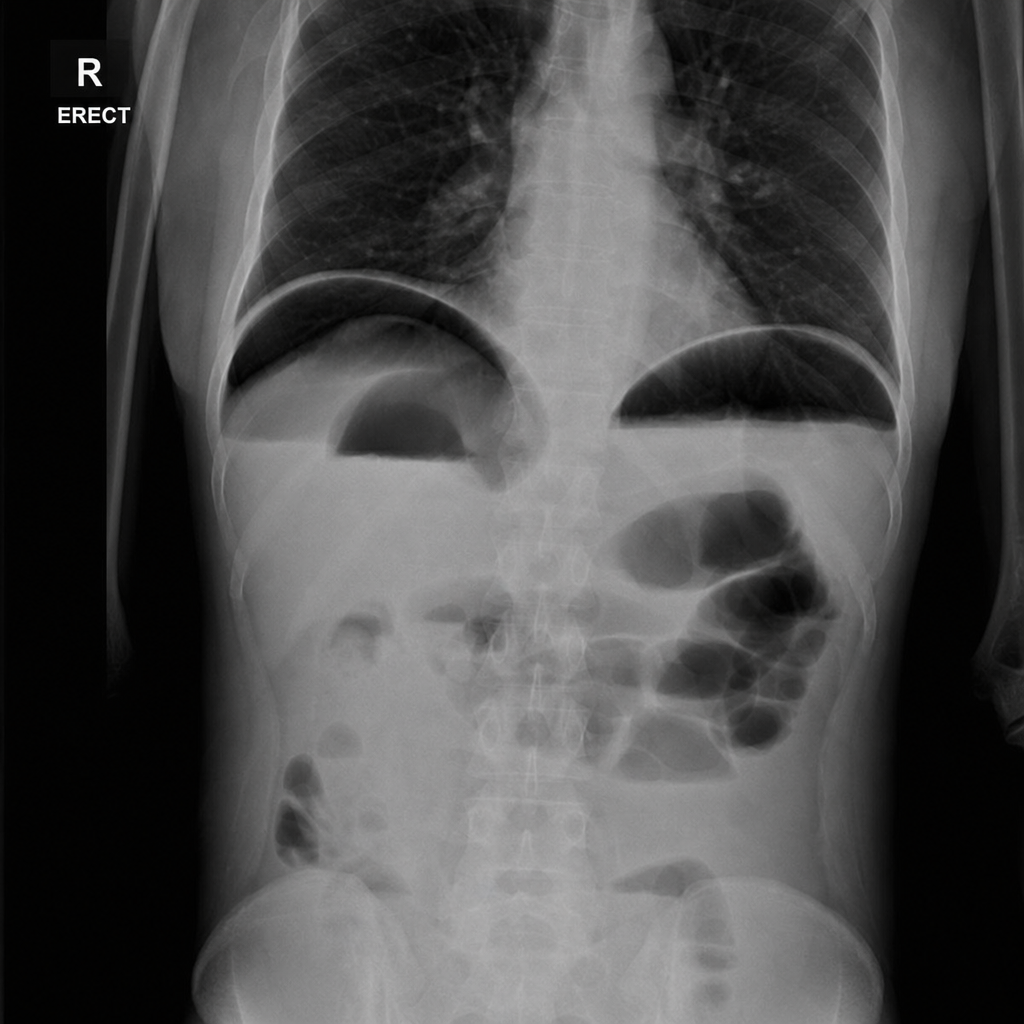
A patient presents with acute abdominal pain with guarding and rigidity. What is the most likely diagnosis?
Which of the following is NOT a feature of paralytic ileus?
What is the aim of preventing reflux esophagitis by repairing a hiatus hernia?
Practice by Chapter
Esophageal Disorders
Practice Questions
Gastric Disorders
Practice Questions
Small Intestine Pathology
Practice Questions
Appendicitis
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Diverticular Disease
Practice Questions
Anorectal Disorders
Practice Questions
Colorectal Neoplasms
Practice Questions
Gastrointestinal Stomas
Practice Questions
Bariatric Surgery Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app