
Gastrointestinal Surgery — MCQs

On this page
What is the most common cause of acute mesenteric ischemia?
Which is the most stable suture layer in all sections of the gastrointestinal tract?
A 65-year-old patient presents with dysphagia and regurgitation. Barium swallow shows diverticula at the lower esophagus. Which of the following statements about this condition is FALSE?
A 50-year-old labourer, a smoker, presented with repeated episodes of epigastric pain, associated with occasional vomiting and weight loss. What is the diagnosis?
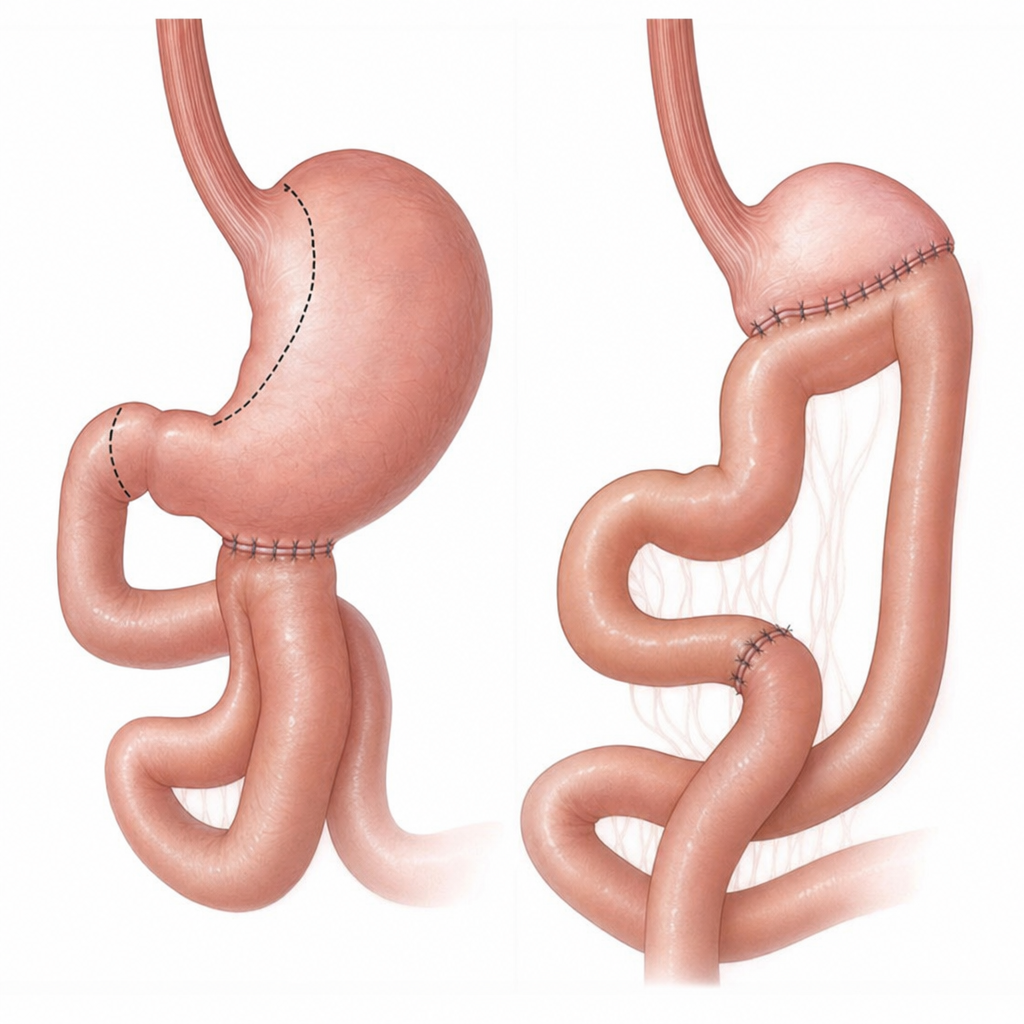
A 40-year-old male patient presents with intractable peptic ulcer disease. The physician recommends a procedure for symptomatic relief, which is depicted in the accompanying image. Which of the following findings is NOT a complication of the procedure performed?
Which of the following is NOT true about appendicitis?
Which of the following is NOT typically performed in the management of an obstructed inguinal hernia?
A 65-year-old man presents with severe bilious vomiting following gastric surgery. In which circumstance does this typically occur?
Which of the following is not a risk factor for squamous cell carcinoma of the esophagus?
What is the most common nerve to get entrapped during open inguinal hernia surgery?
Practice by Chapter
Esophageal Disorders
Practice Questions
Gastric Disorders
Practice Questions
Small Intestine Pathology
Practice Questions
Appendicitis
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Diverticular Disease
Practice Questions
Anorectal Disorders
Practice Questions
Colorectal Neoplasms
Practice Questions
Gastrointestinal Stomas
Practice Questions
Bariatric Surgery Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app