
Gastrointestinal Surgery — MCQs

On this page
What is the most common cause of splenic rupture?
A 32-year-old patient presents with diarrhea and flushing. CT scan reveals multiple lesions in the liver. The primary disease is most likely located in which of the following?
A 37-year-old woman presents with high fever (39.5°C), nausea, and vomiting. Physical examination reveals increased abdominal pain in the paraumbilical region, rebound tenderness over McBurney's point, and a positive psoas sign. Blood tests show marked leukocytosis. What is the most likely diagnosis?
What is true about a femoral hernia?
Which of the following is FALSE about short bowel syndrome?
A 60-year-old female presents with a tender, irreducible mass immediately below and lateral to the pubic tubercle. Plain abdominal X-ray shows intestinal obstruction. What is the most likely diagnosis?
Which is the most common site for a duodenal ulcer?
What is the most important step in the repair of an indirect inguinal hernia?
A 63-year-old man undergoes a partial gastrectomy with Billroth II reconstruction for intractable peptic ulcer disease. He presents several months postoperatively with a megaloblastic anemia. Which of the following is the best treatment for this surgical complication?
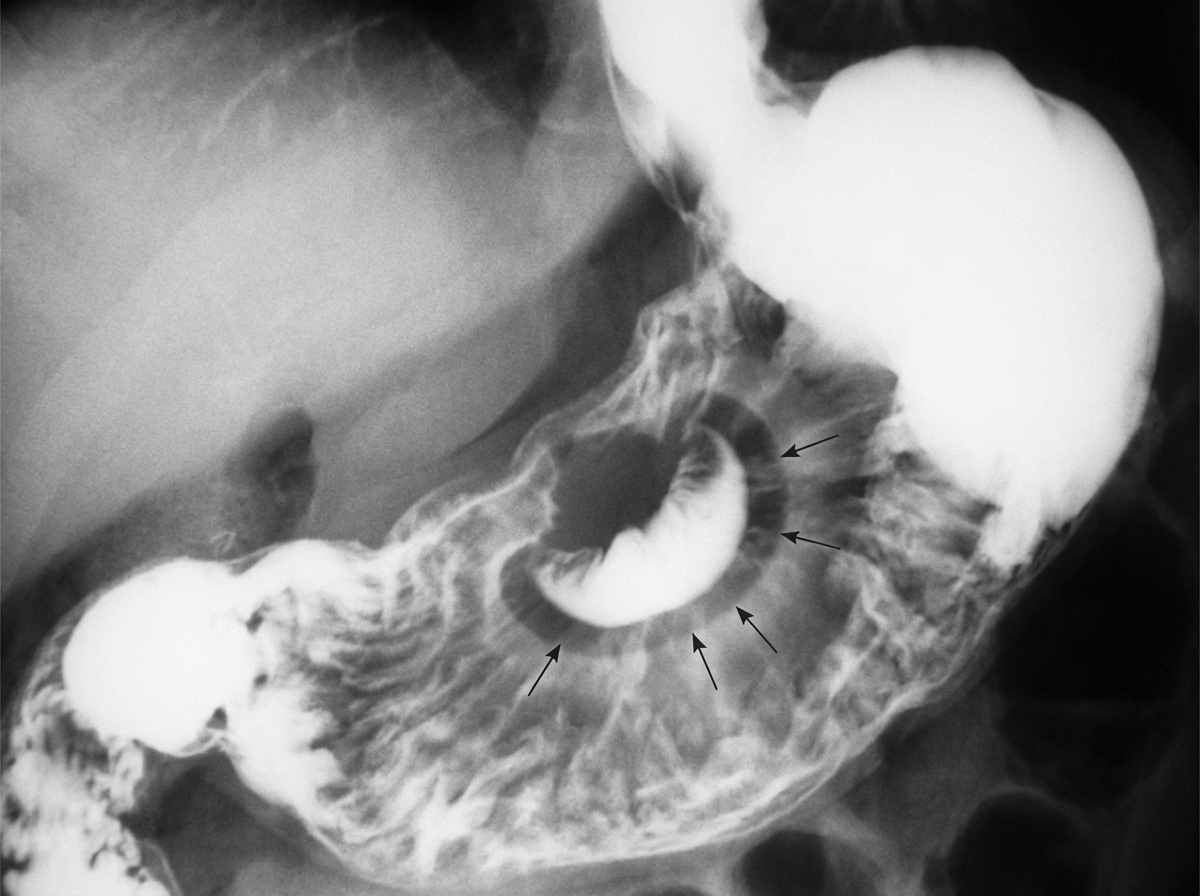
Which condition is diagnosed by the following sign?
Practice by Chapter
Esophageal Disorders
Practice Questions
Gastric Disorders
Practice Questions
Small Intestine Pathology
Practice Questions
Appendicitis
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Diverticular Disease
Practice Questions
Anorectal Disorders
Practice Questions
Colorectal Neoplasms
Practice Questions
Gastrointestinal Stomas
Practice Questions
Bariatric Surgery Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app