
Gastrointestinal Surgery — MCQs

On this page
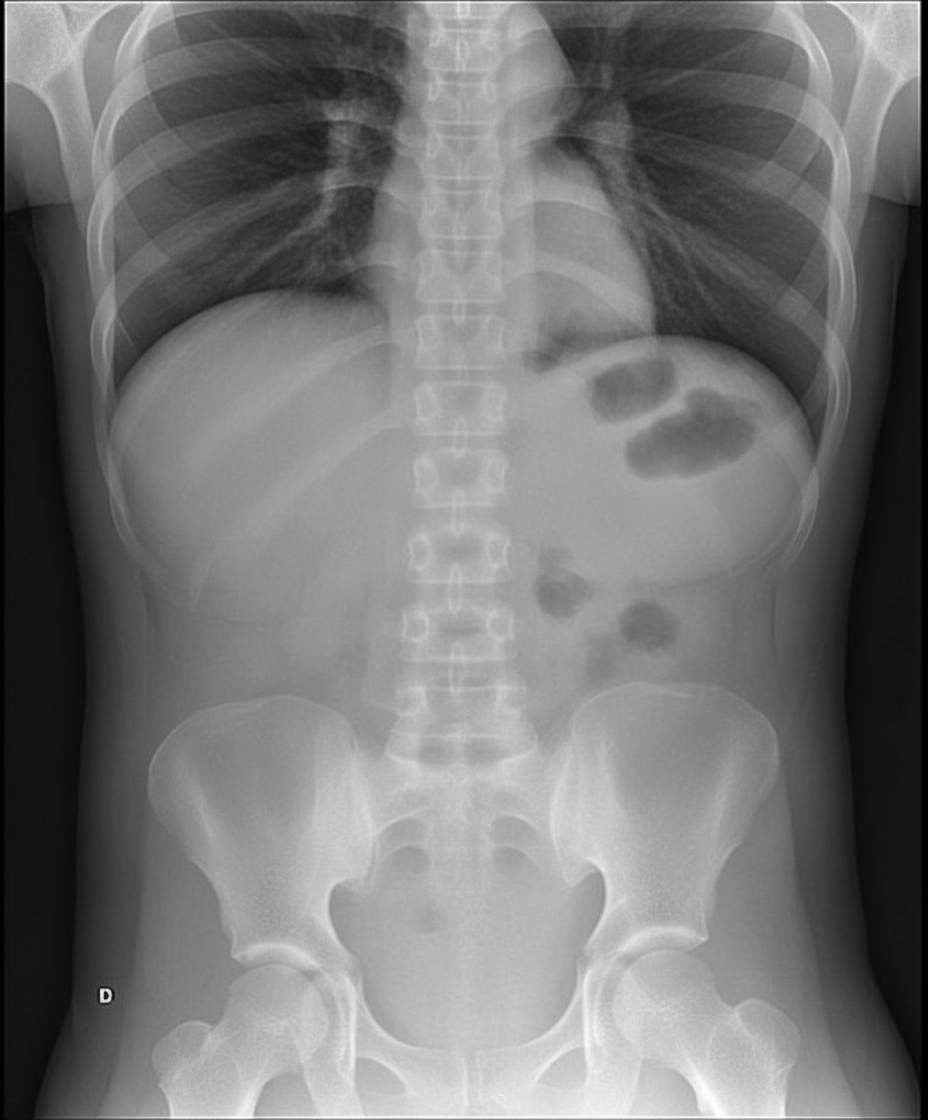
A patient presents with abdominal distention, nausea, and vomiting, reporting a long history of intermittent obstructive symptoms and distention. Radiological examination shows the following presentation. Which of the following statements regarding the treatment of this condition is false?
Which of the following statements about gastric carcinoma is incorrect?
What is the most common nutritional deficiency observed after a gastrectomy?
Howship-Romberg sign is associated with which condition?
Which of the following is true about acute dilatation of the stomach?
A patient presents with hematemesis and melena. An initial upper GI endoscopy reveals no significant findings. Two days later, the patient rebleeds. What is the next appropriate investigation?
Diverticular disease is not common in which part of the gastrointestinal tract?
Dumping syndrome is associated with which of the following?
Which of the following is NOT true about Pseudomyxoma peritonei?
What is true about duodenal adenocarcinoma?
Practice by Chapter
Esophageal Disorders
Practice Questions
Gastric Disorders
Practice Questions
Small Intestine Pathology
Practice Questions
Appendicitis
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Diverticular Disease
Practice Questions
Anorectal Disorders
Practice Questions
Colorectal Neoplasms
Practice Questions
Gastrointestinal Stomas
Practice Questions
Bariatric Surgery Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app