
Gastrointestinal Surgery — MCQs

On this page
All of the following are sequelae of peptic ulcer surgery EXCEPT:
A 38-year-old man with Crohn's disease presents with a 3-day history of increasing abdominal pain, distension, and inability to pass gas or stool. CT shows dilated small bowel loops with a transition point in the terminal ileum and bowel wall thickening. What factor most influences the decision between conservative and surgical management?
A 45-year-old woman undergoes laparoscopic cholecystectomy. On postoperative day 3, she develops right upper quadrant pain, fever, and jaundice. Her bilirubin rises from 1.2 to 8.5 mg/dL. ERCP shows extravasation of contrast from the common bile duct. What is the most likely cause of this complication?
A 25-year-old woman with inflammatory bowel disease requires total colectomy with ileostomy. She is getting married in 6 months and wants to know about conversion to J-pouch. She has mild perianal disease and takes anti-TNF therapy. Evaluate the timing and appropriateness of J-pouch reconstruction.
A 28-year-old woman with ulcerative colitis requires emergency colectomy for toxic megacolon. She is 20 weeks pregnant with her first child. The obstetric team is concerned about fetal risks, while the surgical team emphasizes maternal life-threatening condition. The patient wants to prioritize fetal safety. Evaluate the management approach.
Which of the following is not seen with ileal resections?
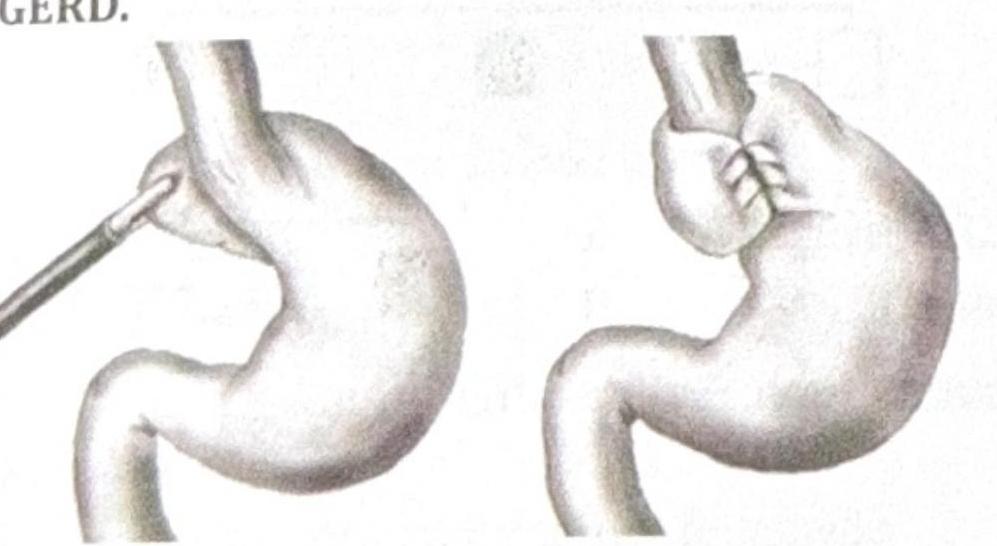
Identify the procedure shown in the image, which is performed in a patient with recurrent GERD.
All the following are true about acute cholecystitis, except
A 34-year-old patient presents with severe pain in the right upper quadrant that radiates to the right shoulder. During laparoscopic cholecystectomy, which of the following anatomical spaces must be carefully identified to prevent bile duct injury?
A 23-year-old man presents to the emergency department with bloody vomitus. The patient is an alcoholic and has presented similarly before. He is given ondansetron; however, he continues to vomit. The patient complains of sudden substernal chest pain and dysphagia after another bout of vomiting. His temperature is 99°F (37.2°C), blood pressure is 117/60 mmHg, pulse is 122/min, respirations are 15/min, and oxygen saturation is 99% on room air. Physical exam is notable for an uncomfortable man with subcutaneous emphysema in the patient’s neck and supraclavicular areas. Which of the following is the most likely diagnosis?
Practice by Chapter
Esophageal Disorders
Practice Questions
Gastric Disorders
Practice Questions
Small Intestine Pathology
Practice Questions
Appendicitis
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Diverticular Disease
Practice Questions
Anorectal Disorders
Practice Questions
Colorectal Neoplasms
Practice Questions
Gastrointestinal Stomas
Practice Questions
Bariatric Surgery Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app