
Gastrointestinal Surgery — MCQs

On this page
Which one of the following parts of intussusception is most susceptible to ischaemia and perforation?
What is the treatment of choice in a patient with Crohn’s disease, where inflamed appendix was found on exploration?
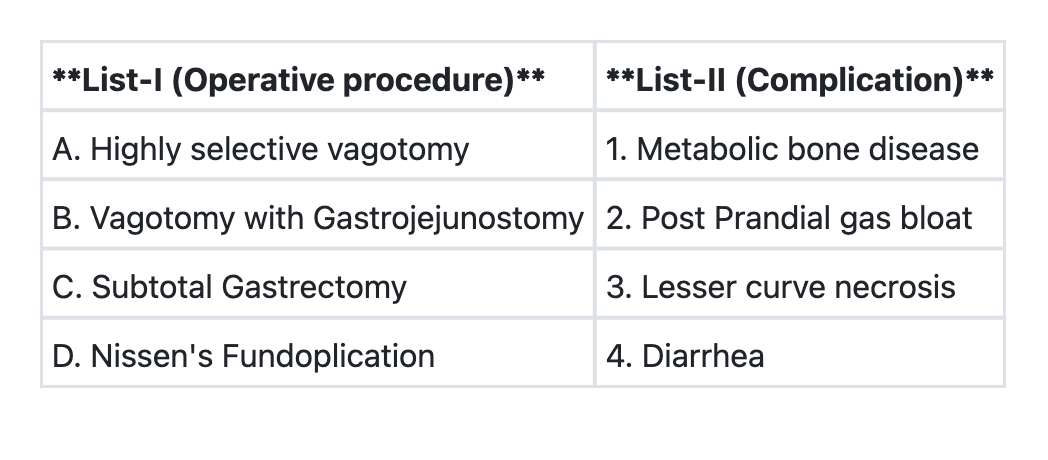
Match List-I with List-II and select the correct answer using the code given below the Lists: **List-I (Procedure)** A. Highly selective vagotomy B. Vagotomy with gastrojejunostomy C. Subtotal gastrectomy D. Nissen's fundoplication **List-II (Complication)** 1. Metabolic bone disease 2. Post-prandial gas bloat 3. Lesser curve necrosis 4. Diarrhea **Code:**
In a patient of gastric outlet obstruction nutritional support is best delivered by:
Mousseau-Barbin Tube (M.B.Tube) is used for:
The most common cause of intestinal obstruction is:
In gallstone ileus, obstruction most frequently occurs at:
A 48 year old male with the history of chronic duodenal ulcer presented in surgical emergency with the complaints of sudden severe pain in the abdomen. At presentation: Pulse = 120/m, BP = 90/60 mm of Hg Abdomen: Tenderness (+), Rigidity (+), Guarding (+) Respiratory Rate: 20/m X-ray: Gas under right dome of diaphragm The probable diagnosis is:
Which of the following is NOT a tissue repair surgery for inguinal hernia repair?
Valentino's syndrome is:
Practice by Chapter
Esophageal Disorders
Practice Questions
Gastric Disorders
Practice Questions
Small Intestine Pathology
Practice Questions
Appendicitis
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Intestinal Obstruction
Practice Questions
Gastrointestinal Bleeding
Practice Questions
Diverticular Disease
Practice Questions
Anorectal Disorders
Practice Questions
Colorectal Neoplasms
Practice Questions
Gastrointestinal Stomas
Practice Questions
Bariatric Surgery Principles
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app