
Endocrine Surgery — MCQs

On this page
A 40-year-old woman with a history of hyperthyroidism undergoes a thyroidectomy. She develops tingling and muscle cramps postoperatively. What complication should be investigated?
A 35-year-old woman with a goiter presents with difficulty swallowing and an ultrasound revealing a 3 cm nodule. What is the most appropriate management?
A patient who underwent thyroidectomy experiences a drop in calcium levels post-operatively. What is the most likely cause?
A 48-year-old woman with a thyroid nodule and elevated calcitonin levels undergoes surgery. Postoperatively, she develops hypocalcemia. What is the likely cause?
A patient with a thyroid nodule undergoes fine-needle aspiration, which reveals a follicular neoplasm. What is the next step?
What surgical procedure is indicated for a patient with symptomatic pheochromocytoma?
A 35-year-old female with a history of Graves' disease is scheduled for a total thyroidectomy. Which of the following strategies is the most critical to minimize complications during the procedure?
A patient undergoing a thyroidectomy is at risk of hypocalcemia post-operation due to the accidental removal of which glands?
Which of the following statements about retrosternal goiter is correct?
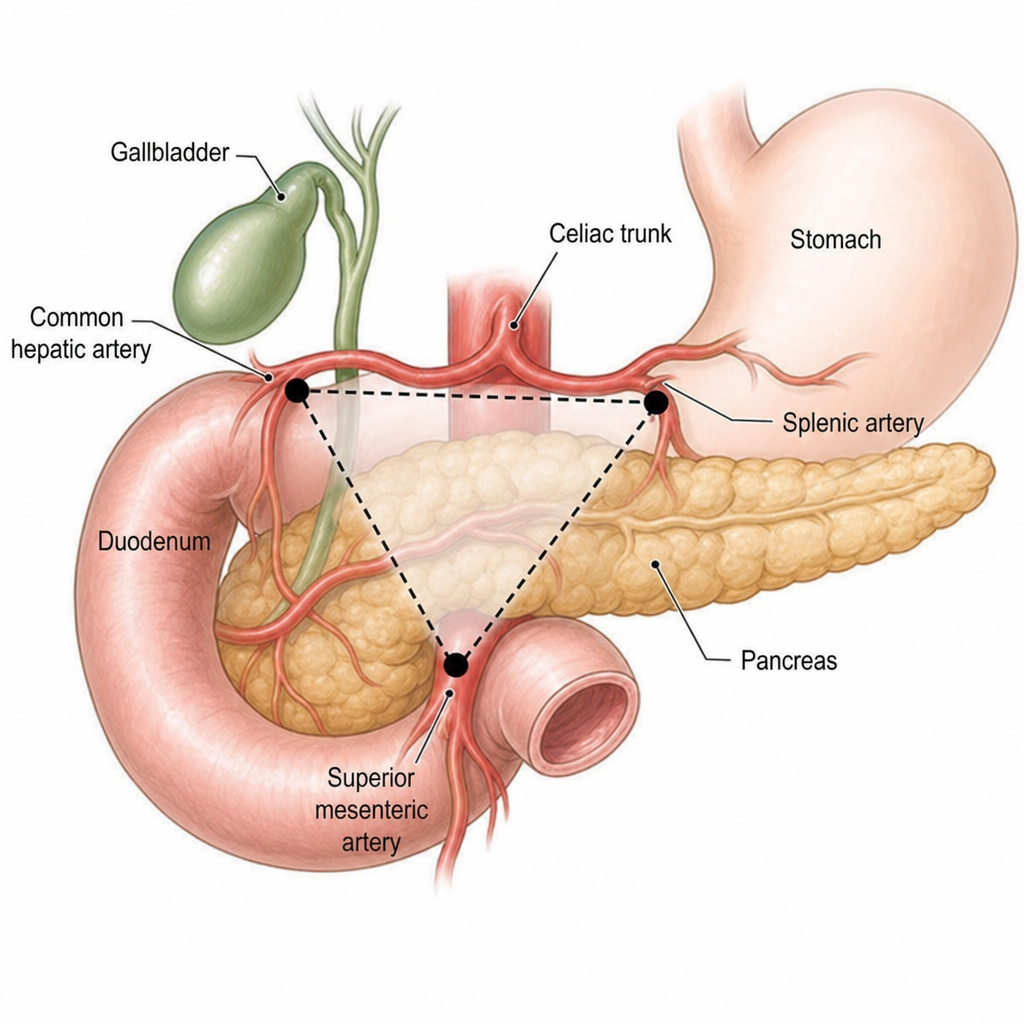
Identify the triangle in the image below.
Practice by Chapter
Thyroid Nodules
Practice Questions
Thyroid Cancer
Practice Questions
Graves' Disease
Practice Questions
Thyroiditis
Practice Questions
Primary Hyperparathyroidism
Practice Questions
Secondary and Tertiary Hyperparathyroidism
Practice Questions
Adrenal Cortical Tumors
Practice Questions
Pheochromocytoma
Practice Questions
Adrenal Incidentalomas
Practice Questions
Multiple Endocrine Neoplasia
Practice Questions
Neuroendocrine Tumors
Practice Questions
Intraoperative Monitoring in Endocrine Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app