
Endocrine Surgery — MCQs

On this page
A 50-year-old woman after thyroidectomy comes to you for a 2nd opinion for further treatment of papillary thyroid cancer. What would you recommend for this patient?
Multiple lytic lesions on skull are seen in which thyroid carcinoma?
Based on the provided X-ray image showing lytic bone lesions in the skull, which thyroid carcinoma classically spreads hematogenously to bone?
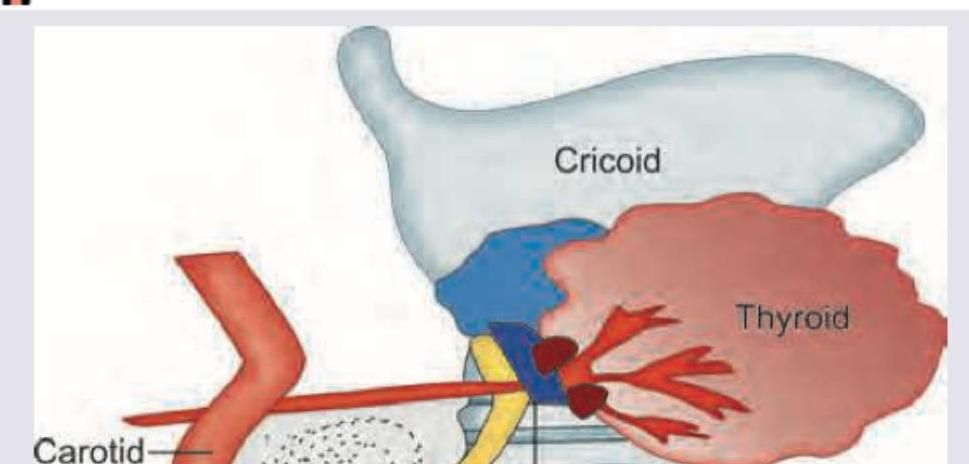
What is the triangle shown in the figure known as?
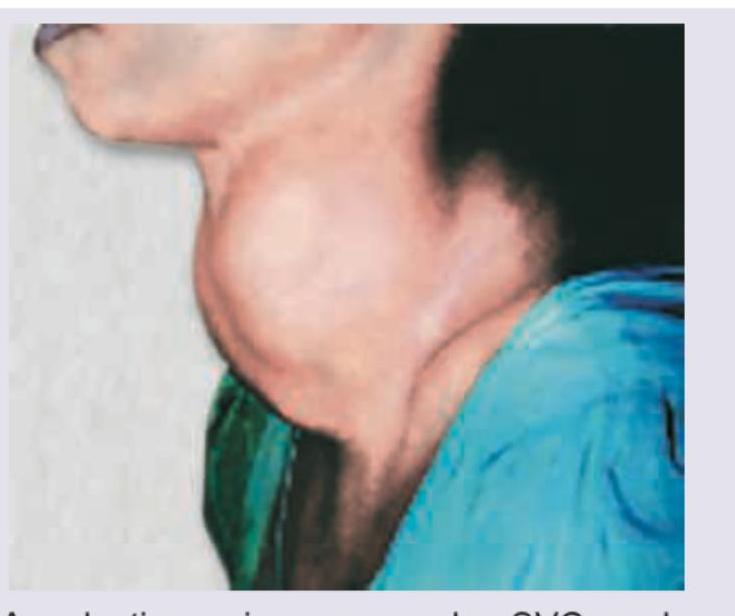
A 35-year-old female presents with a large thyroid swelling. Her chest X-ray is shown below. What is the most likely diagnosis?

The image shows a large multinodular goiter with bosselated appearance. Which amongst the following is commonly seen in this patient?
Which of the following statements regarding Thyroglossal duct are correct ? 1. It is situated in midline of neck. 2. It moves upwards on swallowing but not on tongue protrusion. 3. It is treated with Sistrunk operation. 4. It may be the only functioning thyroid tissue in the body. Select the correct answer using the code given below :
A 60-year-old lady presents with a recent onset increase in a long standing swelling on the front of the neck. The swelling, which was small, had been present since last 30 years, but has now increased to more than twice the size in the last 2 months. On examination, the swelling is firm to hard in consistency and moves with deglutition. What is the most likely cause of this clinical presentation?
A midline neck swelling just below the hyoid bone and managed by Sistrunk's operation leads to postoperative need for thyroxine replacement. The most likely diagnosis is
Surgical treatment for a 40-years old lady with 3 x 3 cm. papillary carcinoma thyroid with level III enlarged lymph nodes is :
Practice by Chapter
Thyroid Nodules
Practice Questions
Thyroid Cancer
Practice Questions
Graves' Disease
Practice Questions
Thyroiditis
Practice Questions
Primary Hyperparathyroidism
Practice Questions
Secondary and Tertiary Hyperparathyroidism
Practice Questions
Adrenal Cortical Tumors
Practice Questions
Pheochromocytoma
Practice Questions
Adrenal Incidentalomas
Practice Questions
Multiple Endocrine Neoplasia
Practice Questions
Neuroendocrine Tumors
Practice Questions
Intraoperative Monitoring in Endocrine Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app