
Endocrine Surgery — MCQs

On this page
A 26-year-old woman presents with a palpable thyroid nodule. Needle biopsy demonstrates amyloid in the stroma of the lesion. A cervical lymph node is palpable on the same side as the lesion. What is the preferred treatment?
A patient presents with a small solitary nodule in the right lobe of the thyroid. FNAC shows follicular adenoma. What is the best surgical management?
Postoperative hypoparathyroidism-related hypocalcemia usually presents within what timeframe?
A patient develops sudden respiratory distress in the postoperative room after thyroid surgery. The dressing is removed and found to be slightly blood-stained with a bulging wound. What is the first action to be taken?
Which of the following are indications for surgery in a case of thyroid swelling?
Which of the following is NOT a feature of medullary carcinoma of the thyroid?
A patient with multinodular goiter developed pain and difficulty in breathing. Which of the following types of thyroid carcinoma is most likely to cause this complication?
What is the approximate amount of thyroid tissue typically left on each side after a subtotal thyroidectomy?
What is the stage of an adrenocortical carcinoma measuring 6cm without invasion of surrounding structures?
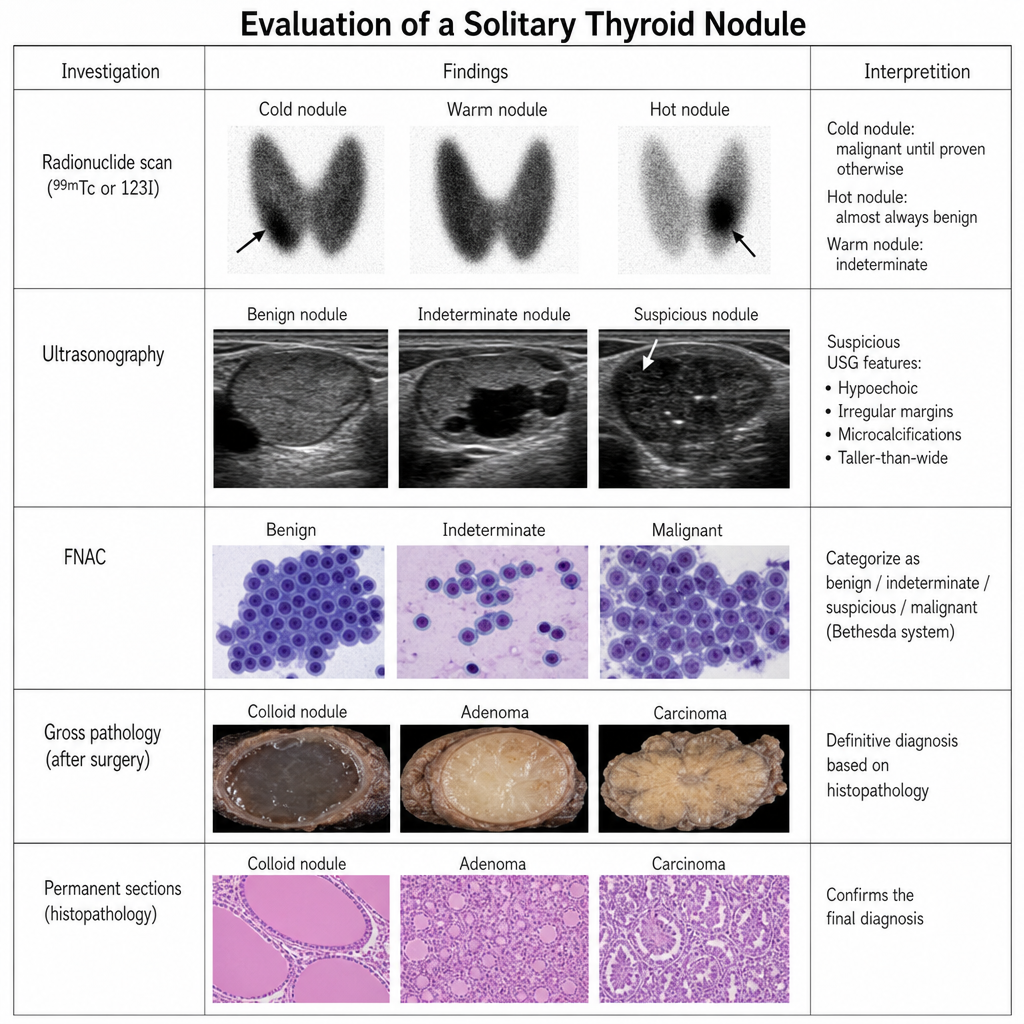
Which of the following statements about a solitary thyroid nodule are TRUE? 1. Most solitary nodules are malignant. 2. Hot nodules on scintigraphy are likely to be malignant. 3. FNAC can reliably distinguish between follicular adenoma and carcinoma. 4. Ultrasound is the most sensitive tool for detecting nodules. 5. The first step in evaluation is TSH levels.
Practice by Chapter
Thyroid Nodules
Practice Questions
Thyroid Cancer
Practice Questions
Graves' Disease
Practice Questions
Thyroiditis
Practice Questions
Primary Hyperparathyroidism
Practice Questions
Secondary and Tertiary Hyperparathyroidism
Practice Questions
Adrenal Cortical Tumors
Practice Questions
Pheochromocytoma
Practice Questions
Adrenal Incidentalomas
Practice Questions
Multiple Endocrine Neoplasia
Practice Questions
Neuroendocrine Tumors
Practice Questions
Intraoperative Monitoring in Endocrine Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app