
Colorectal Surgery — MCQs

On this page
What is the recommended treatment for squamous cell carcinoma of the anal canal in a 46-year-old healthy man who does not require a colostomy?
All of the following are common features of hemorrhoids except?
What is the condition for which the treatment shown below is followed?
A 40-year-old male patient presented with mild abdominal pain, mild constipation with a feeling of incomplete evacuation, and mucus in stools for the past 4 years. On examination, tenderness is present in the left iliac fossa. What is the most likely diagnosis?
Five-day self-subsiding pain is diagnostic of?
What is the initial management for rectosigmoid obstructive carcinoma in an elderly frail patient?
A 30-year-old patient presents with loose stools, lower abdominal pain, weight loss, diarrhea, and passage of blood and mucus. Sigmoidoscopy reveals a characteristic presentation. All of the following statements regarding this condition are true EXCEPT?
Which of the following conditions does NOT typically present with bleeding per rectum?
The Karydakis procedure is used for which condition?
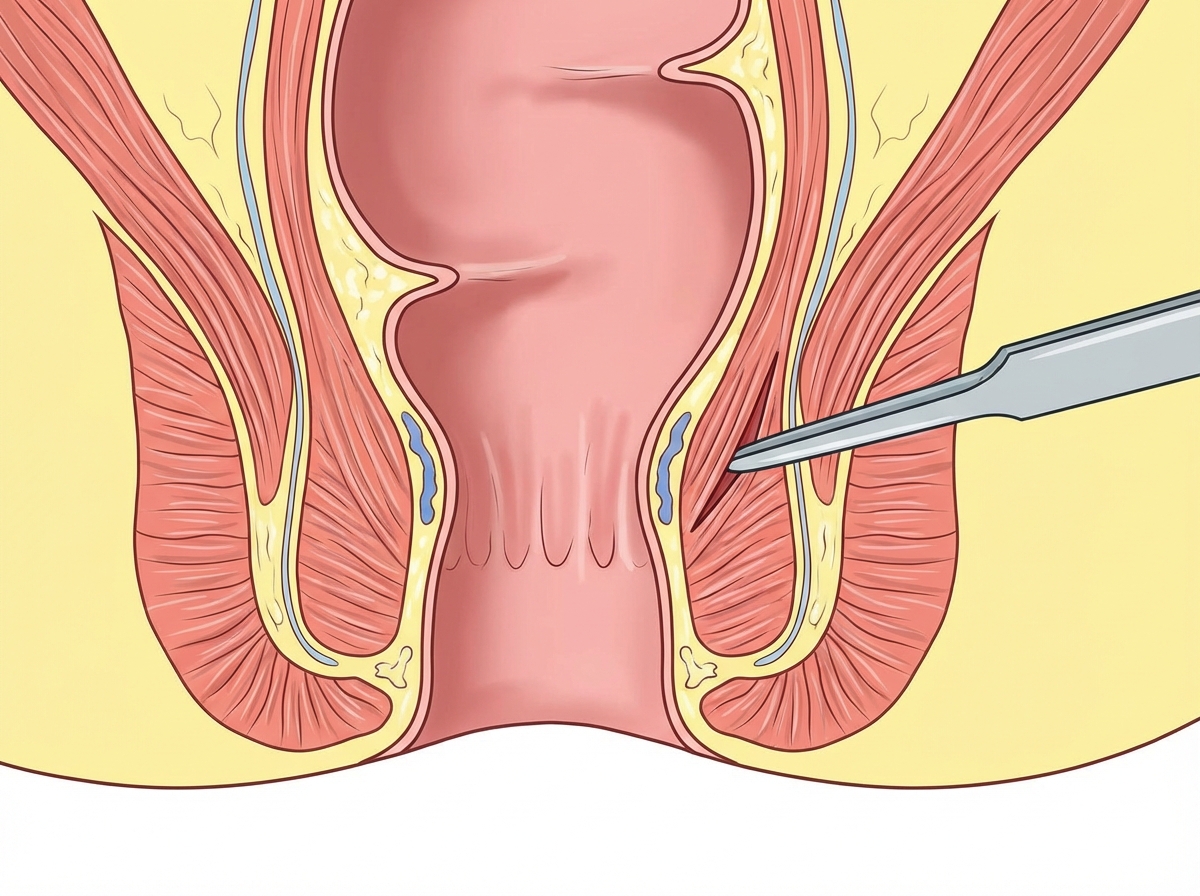
The image below shows a perianal abscess located superficial to the external anal sphincter. How will you drain this abscess?

Practice by Chapter
Colorectal Anatomy and Physiology
Practice Questions
Diverticular Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
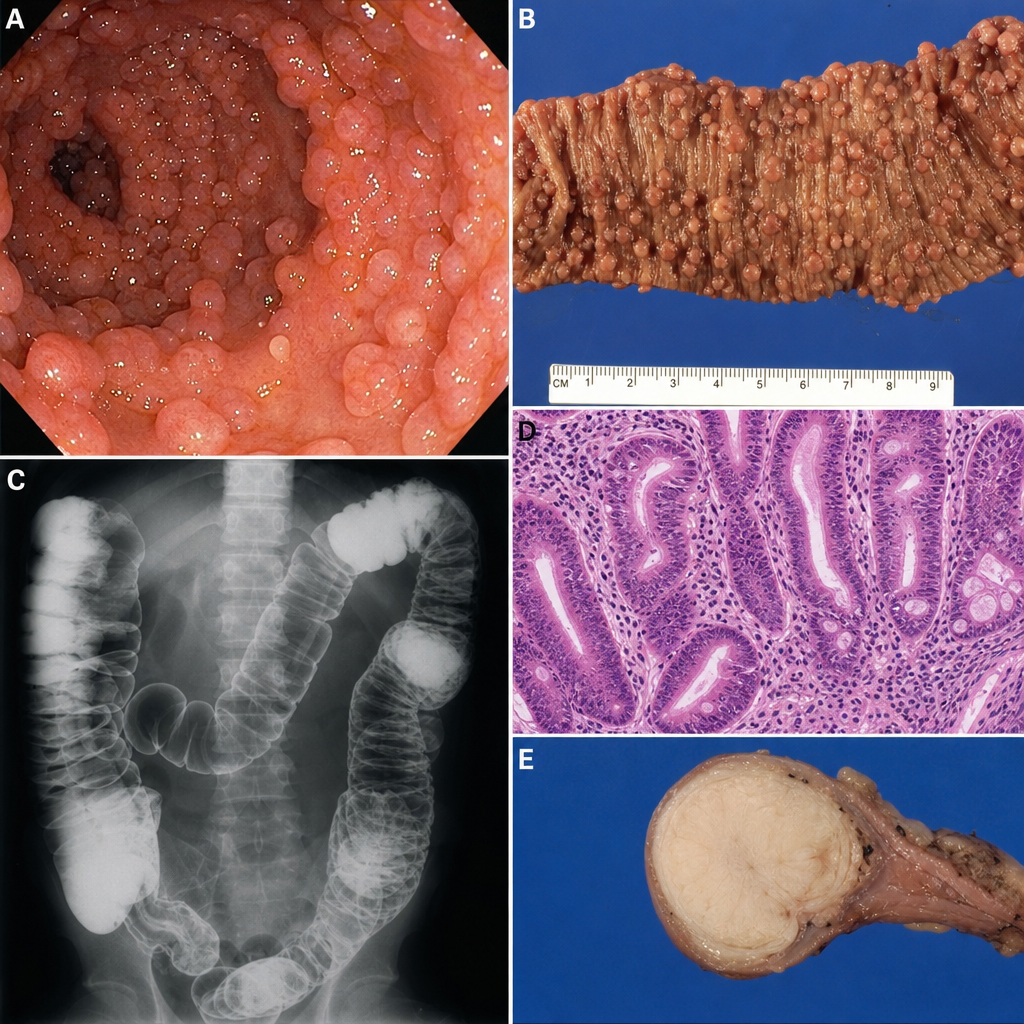
Colorectal Polyps
Practice Questions
Colorectal Cancer
Practice Questions
Anorectal Abscess and Fistula
Practice Questions
Hemorrhoids
Practice Questions
Rectal Prolapse
Practice Questions
Fecal Incontinence
Practice Questions
Intestinal Stomas Creation and Management
Practice Questions
Pelvic Floor Disorders
Practice Questions
Enhanced Recovery After Colorectal Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app