
Colorectal Surgery — MCQs

On this page
Gentleman of 56 years underwent laparoscopic left hemicolectomy for diagnosed left colonic carcinoma. Histopathology revealed the tumour to be invading submucosa and muscularis propria. Among the 16 regional lymph nodes harvested, 2 were positive for malignant deposits. His staging as per AJCC will be:
A 25-year-old woman with inflammatory bowel disease requires total colectomy with ileostomy. She is getting married in 6 months and wants to know about conversion to J-pouch. She has mild perianal disease and takes anti-TNF therapy. Evaluate the timing and appropriateness of J-pouch reconstruction.
A 28-year-old woman with ulcerative colitis requires emergency colectomy for toxic megacolon. She is 20 weeks pregnant with her first child. The obstetric team is concerned about fetal risks, while the surgical team emphasizes maternal life-threatening condition. The patient wants to prioritize fetal safety. Evaluate the management approach.
A 35-year-old HIV-positive woman (CD4 count 180/μL, on HAART) develops extensive perianal condyloma acuminata resistant to conventional treatments. HPV typing shows type 16. What is the most appropriate management approach?
A jeep driver presents with pain in the gluteal region along with swelling and pus discharge for the past 6 months. What is the most likely diagnosis?
What surgery is shown here in the image?
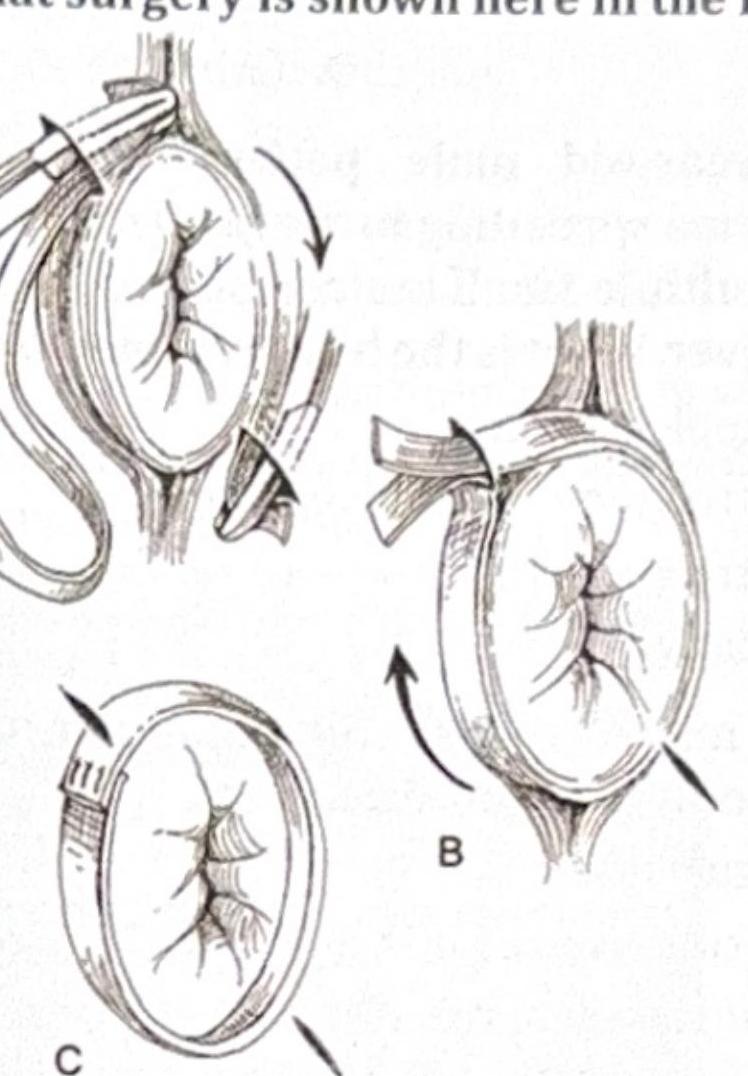
Which of the following is not a perineal approach for the condition shown in the image?

A 53-year-old patient presents with per rectal bleeding. Which is the most appropriate investigation to evaluate for colorectal pathology?
A 56-year-old man is brought to the emergency department for the evaluation of a 3-day history of left lower abdominal pain. During this period, the patient has also had a low-grade fever and has not had a bowel movement. He has a history of constipation. He underwent a cholecystectomy at the age of 53 years. He has smoked one pack of cigarettes daily for the last 30 years. His temperature is 38.8°C (101.8°F), pulse is 80/min, respirations are 18/min, and blood pressure is 130/84 mm Hg. Cardiopulmonary examination shows no abnormalities. Abdominal examination shows left lower quadrant tenderness with no guarding or rebound. There is no edema of his lower extremities. CT of the abdomen with contrast shows segmental wall thickening of the descending colon with multiple diverticula, surrounding fat stranding, and a 5.5-cm, low-attenuating pelvic fluid collection. Intravenous fluids and bowel rest are started. Treatment with intravenous morphine, ciprofloxacin, and metronidazole is begun. Which of the following is the most appropriate next step in the management of this patient?
Best treatment strategy for carcinoma of the anal canal:
Practice by Chapter
Colorectal Anatomy and Physiology
Practice Questions
Diverticular Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Colorectal Polyps
Practice Questions
Colorectal Cancer
Practice Questions
Anorectal Abscess and Fistula
Practice Questions
Hemorrhoids
Practice Questions
Rectal Prolapse
Practice Questions
Fecal Incontinence
Practice Questions
Intestinal Stomas Creation and Management
Practice Questions
Pelvic Floor Disorders
Practice Questions
Enhanced Recovery After Colorectal Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app