
Colorectal Surgery — MCQs

On this page
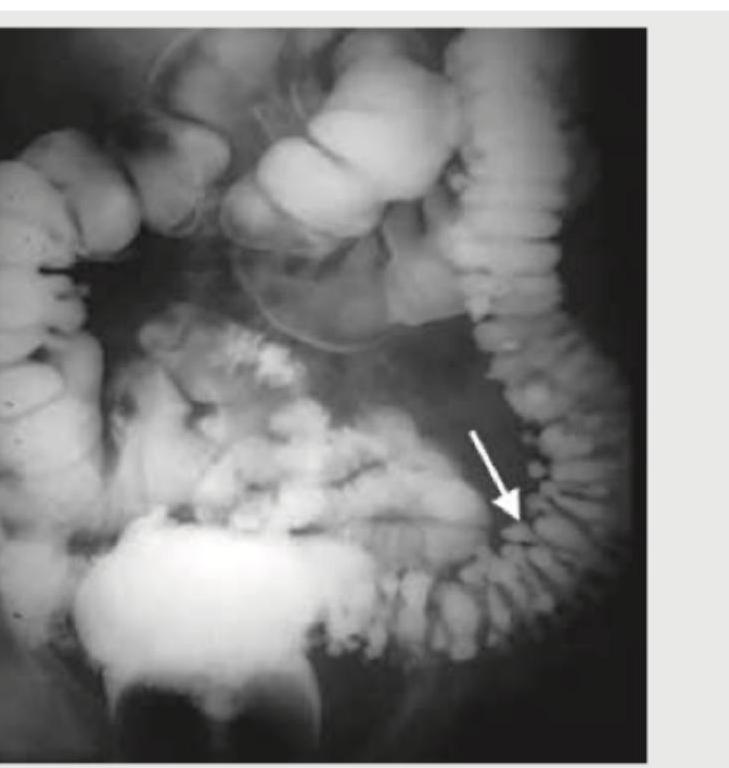
All of the following statements regarding this image are true except:
A 47-year-old man comes to Surgery OPD with history of recurrent episodes of UTI. He gives history of the urine being frothy and occasionally having bubbles. The probable diagnosis is :
Which of the following statements with regard to Colorectal Carcinoma are correct ? 1. Left-sided Colorectal Carcinoma presents with bleeding per rectum. 2. Right-sided Colorectal Carcinoma presents with iron deficiency anaemia. 3. Right-sided Colorectal Carcinoma is more common as compared to the left-sided Colorectal Carcinoma. 4. Colonoscopy is the investigation of choice for suspected Colorectal Carcinoma. Select the correct answer using the code given below :
Which one of the following statements is true regarding "injection sclerotherapy" for haemorrhoids ?
In a 65 year old, double contrast barium enema shows cancer of colon with an apple core appearance. Colonoscopic biopsy shows adenocarcinoma. What will be the next step of management?
A 45 year old underwent surgery for rectal prolapse. At present, he complains of sexual dysfunction which is probably due to the injury of:
A 22 year old young man came with history of occasional bleeding per rectum. On colonoscopy, numerous sessile polyps were seen in descending and sigmoid colon. On family history his elder brother was operated for thyroid malignancy. The young man should be advised:
A colonic carcinoma involving muscularis propria, with one or two nodes involved with a solitary metastasis in the liver, the TNM stage would be:
A 52 year old male patient comes with history of rectal bleeding, alteration in bowel habits and tenesmus. The ideal investigation would be:
A 60 year old male presents with bleeding per rectum. Proctoscopy reveals 2nd degree hemorrhoids. The treatment of choice is:
Practice by Chapter
Colorectal Anatomy and Physiology
Practice Questions
Diverticular Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Colorectal Polyps
Practice Questions
Colorectal Cancer
Practice Questions
Anorectal Abscess and Fistula
Practice Questions
Hemorrhoids
Practice Questions
Rectal Prolapse
Practice Questions
Fecal Incontinence
Practice Questions
Intestinal Stomas Creation and Management
Practice Questions
Pelvic Floor Disorders
Practice Questions
Enhanced Recovery After Colorectal Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app