
Colorectal Surgery — MCQs

On this page
Identify the instrument in the image:
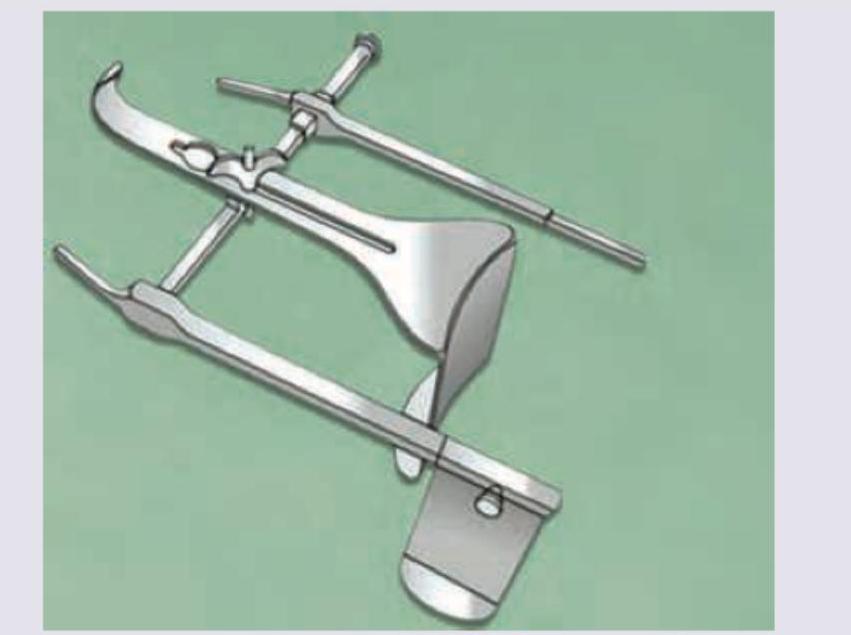
Identify the surgical instrument shown in the image:

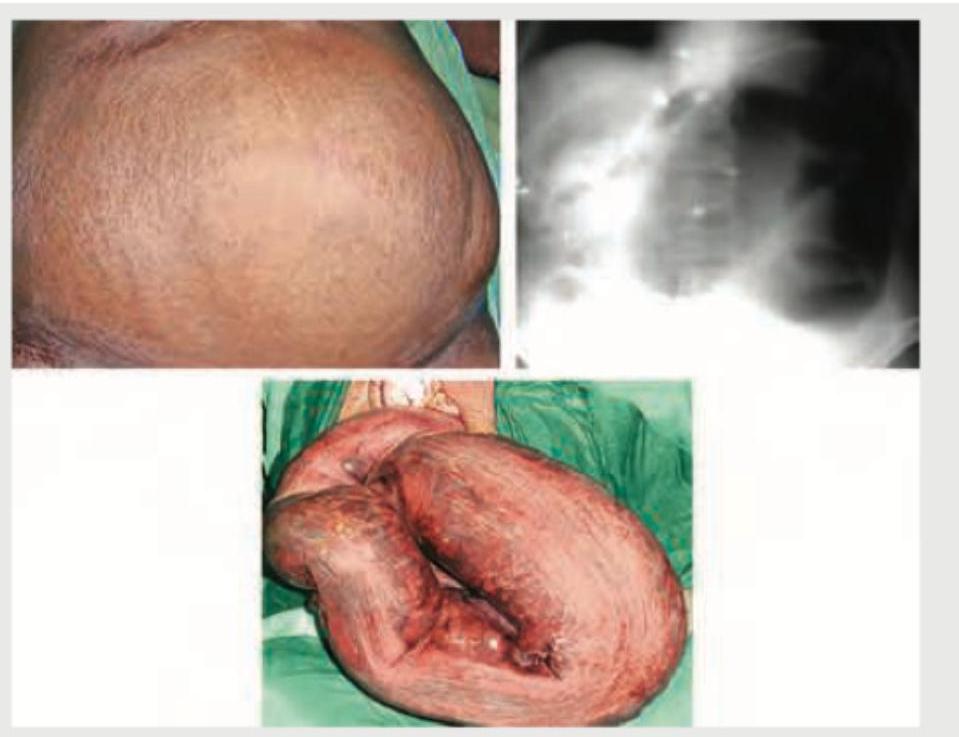
The diagnosis of this patient with left-sided abdominal pain and tyre-like feel of abdomen is?

A patient presents with a biopsy-confirmed squamous cell carcinoma of the anal canal (T2N0M0). What is the preferred treatment for the shown lesion?
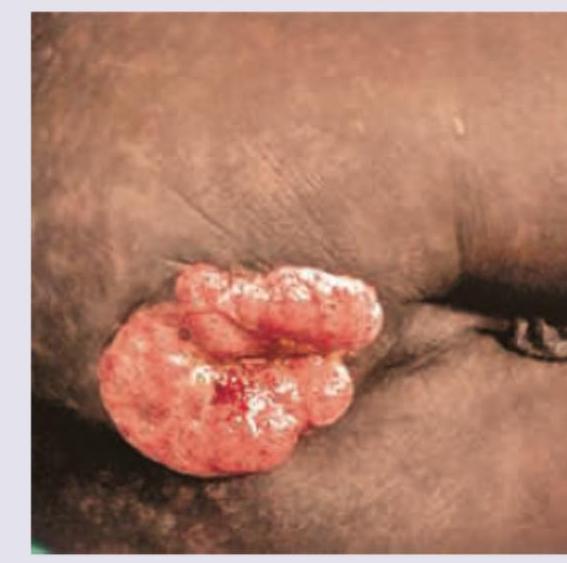
A 29-year-old male who is a doctor by profession, gives a history of prolonged sitting in his OPD hours and presents with discharge and pain. Clinical presentation of the patient is given in the image. What is the most likely diagnosis?

Rectal prolapse occurs due to all EXCEPT:

Which of the following is shown in the image?

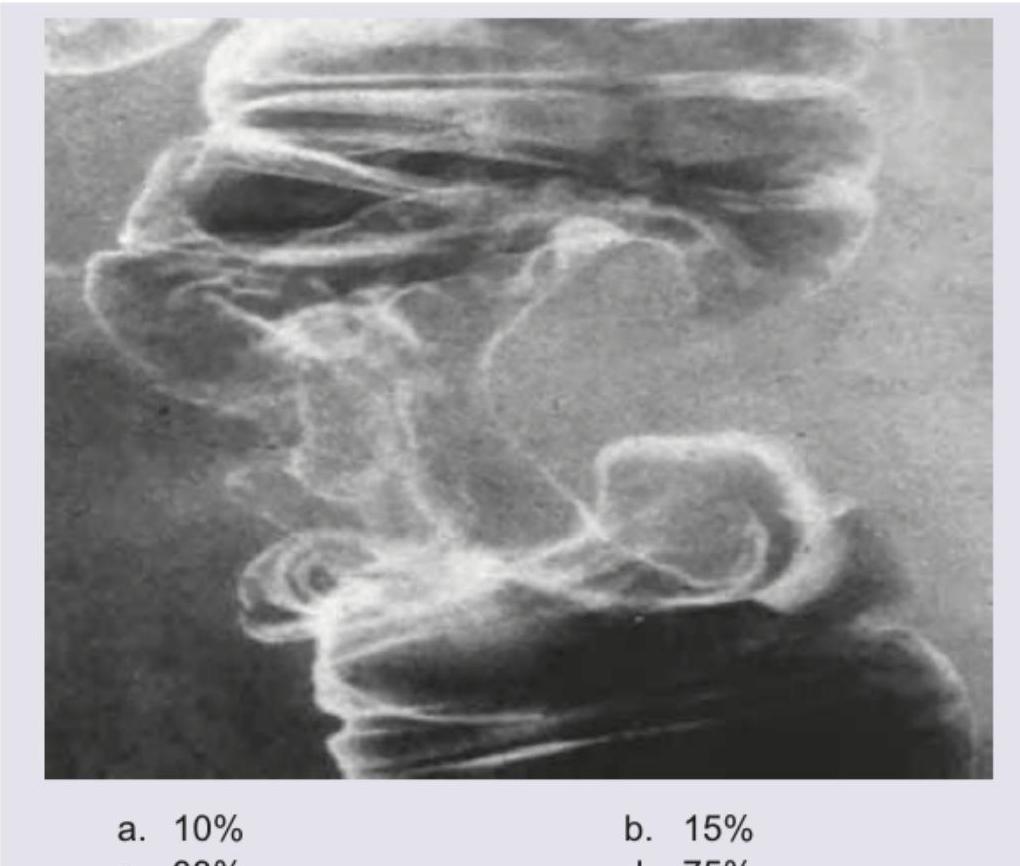
A 35-year-old patient with history of significant weight loss and medically refractory constipation underwent a barium enema shown below. In how many % of cases is synchronous Metastatic liver disease found at the time of colorectal cancer diagnosis?
An 80-year-old male patient complains of bleeding per rectum with alteration in bowel habits. On physical examination of the abdomen there is mass on the left side. Patient's history is positive for smoking, alcohol and regular nonvegetarian food. Barium enema of the patient is given in the below picture. All of the following statements regarding the diagnosis are true except: (Recent NEET Pattern 2016-17)
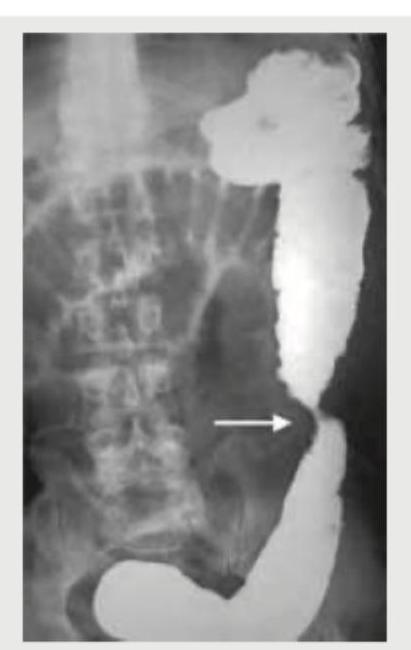
A patient presents with abdominal distension, obstipation and vomiting. The patient reports a long history of intermittent obstructive symptoms and distension. On radiological examination this is the presentation of the patient. Which of the following statement regarding his condition would be false?
Practice by Chapter
Colorectal Anatomy and Physiology
Practice Questions
Diverticular Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Colorectal Polyps
Practice Questions
Colorectal Cancer
Practice Questions
Anorectal Abscess and Fistula
Practice Questions
Hemorrhoids
Practice Questions
Rectal Prolapse
Practice Questions
Fecal Incontinence
Practice Questions
Intestinal Stomas Creation and Management
Practice Questions
Pelvic Floor Disorders
Practice Questions
Enhanced Recovery After Colorectal Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app