
Colorectal Surgery — MCQs

On this page
What is the most common site of perforation during colonoscopy?
Per rectum examination is not a useful test for the diagnosis of which of the following conditions?
A 33-year-old male presents with sudden onset acute abdominal pain, constipation for 1 day, persistent hiccups, and occasional vomiting. An abdominal X-ray was performed. Identify the pathology.
A 70-year-old patient presents with absolute constipation and abdominal distension. The X-ray abdomen is given below. What is the most likely diagnosis?
A patient with grade 2 hemorrhoids underwent surgery, identify the instrument.
A homosexual man complains of painful defecation and mass protruding from the anal canal. Biopsy reveals squamous cell carcinoma of anus. Correct management for this patient is
A man came with complaints of recurrent discharge and pain due to lesions around the anus for 3 years. A diagnosis of fistula-in-ano is made. What is the gold standard investigation for this condition?
A 65-year-old patient undergoes colonoscopy for altered bowel habits. A 6 cm colonic mass is biopsied and histopathology shows adenocarcinoma confined to the mucosa with no lymph node or distant metastasis. What is the most appropriate TNM stage of this tumor?
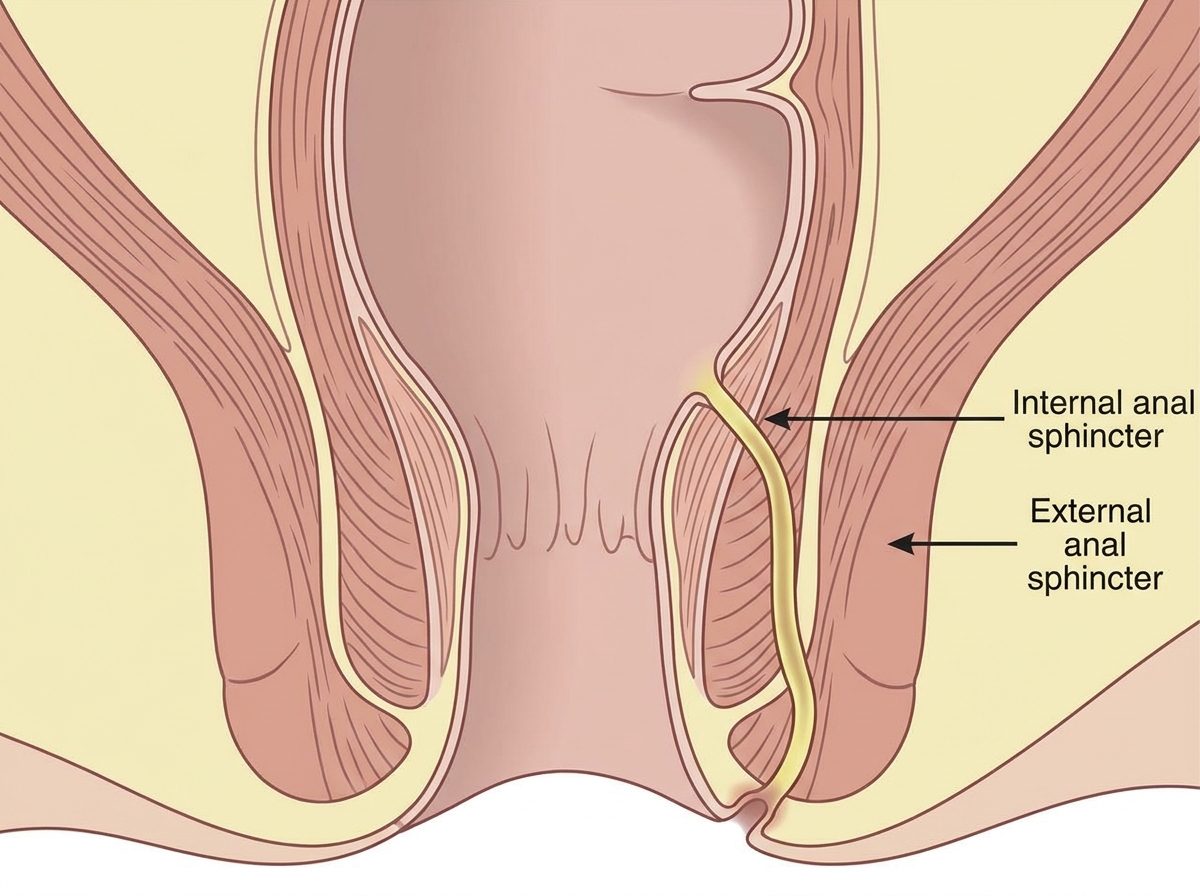
Identify the fistula according to Park's classification?
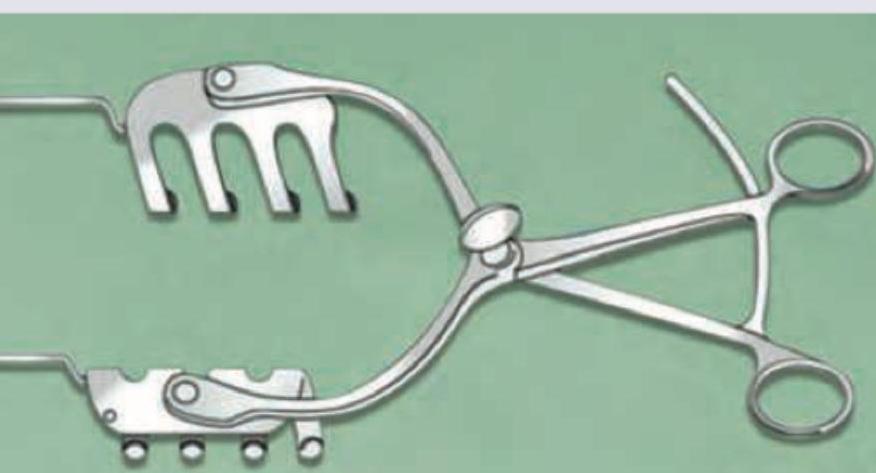
Identify the instrument in the image:
Practice by Chapter
Colorectal Anatomy and Physiology
Practice Questions
Diverticular Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Colorectal Polyps
Practice Questions
Colorectal Cancer
Practice Questions
Anorectal Abscess and Fistula
Practice Questions
Hemorrhoids
Practice Questions
Rectal Prolapse
Practice Questions
Fecal Incontinence
Practice Questions
Intestinal Stomas Creation and Management
Practice Questions
Pelvic Floor Disorders
Practice Questions
Enhanced Recovery After Colorectal Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app