
Colorectal Surgery — MCQs

On this page
A patient is planned for elective colon surgery. What is the ideal timing for administration of prophylactic parenteral antibiotics?
A 65-year-old male with diabetes mellitus presents with purulent rectal discharge and is diagnosed with fistula-in-ano. Surgical management is planned. Which of the following procedures is considered internal anal sphincter-preserving?
What is the fundamental surgical principle underlying TME in the operative management of rectal cancer?
According to the American Association for the Surgery of Trauma (AAST) colon injury grading scale, how is a colonic laceration involving more than 50% of the bowel wall circumference without complete transection classified?
On defecography, a rectocele is considered clinically significant when there is anterior bulging of the rectal wall into the posterior vaginal wall measuring more than:
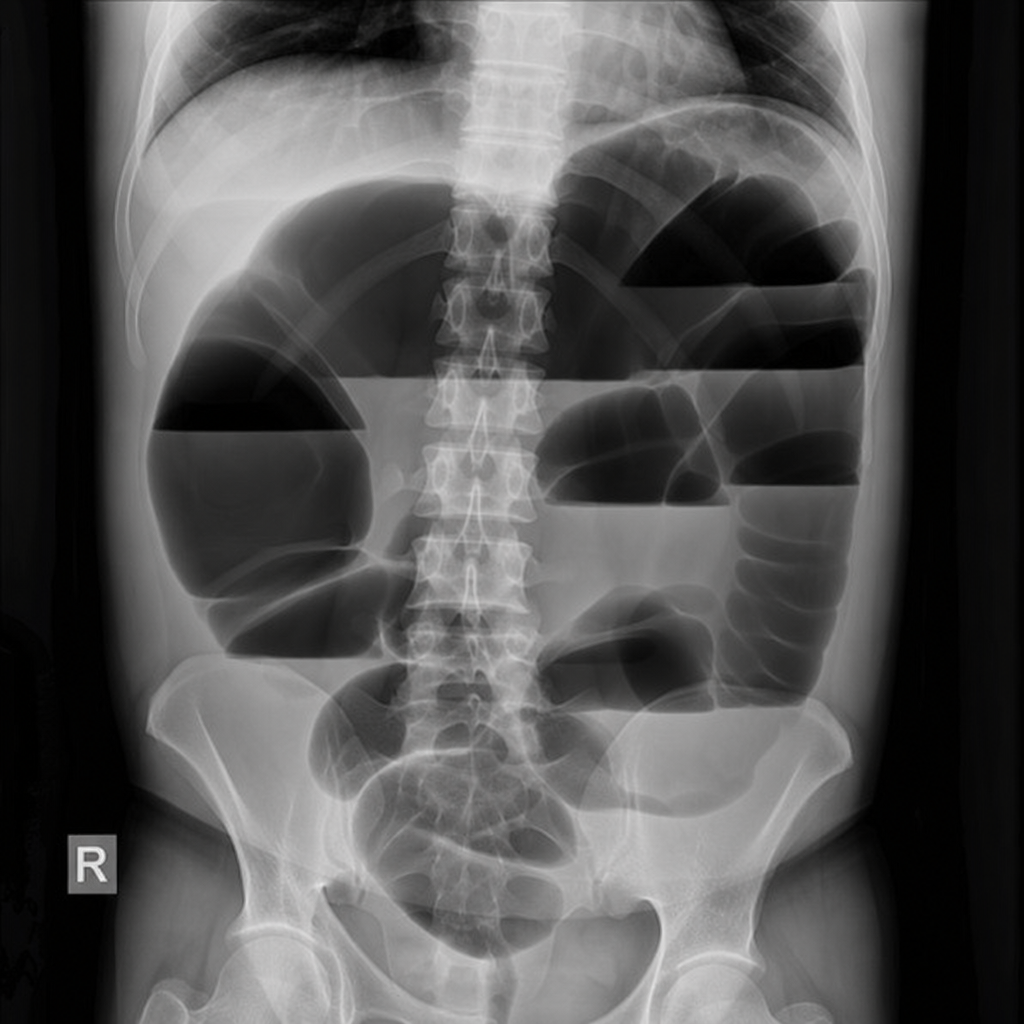
A 65-year-old male with chronic constipation and a history of psychiatric institutionalisation presents with sudden-onset abdominal distension and absolute constipation for 48 hours. He has mild diffuse tenderness without peritoneal signs. HR 102 bpm, BP 118/74 mmHg, afebrile. His plain abdominal X-ray is shown (Image 1). What is the most appropriate next step in management?

A 65-year-old man with chronic constipation and a history of psychiatric illness presents to the emergency department with sudden-onset abdominal distension, absolute constipation for 48 hours, and colicky central abdominal pain. His abdomen is tympanitic on percussion. Vital signs are stable. The plain erect abdominal X-ray is shown in Image 2. There is no peritonism on examination. What is the most appropriate initial management?
A 62-year-old woman presents with a 4-month history of altered bowel habit, passage of blood mixed with stool, and a 6 kg unintentional weight loss. Colonoscopy was attempted but could not be completed due to a near-obstructing lesion in the descending colon. Her haemoglobin is 9.2 g/dL with a microcytic picture. She is clinically stable with no abdominal distension, peritonitis, or complete bowel obstruction. The barium enema is shown in Image 1. Staging CT confirms the lesion is confined to the bowel wall with no nodal or distant metastases (T2N0M0). Which of the following is the most appropriate surgical procedure?

A 60-year-old male presented with bleeding per rectum. On digital rectal examination, a growth was palpable at the tip of the index finger. Sigmoidoscopy revealed an ulcero-proliferative growth located 6 cm from the anal verge. CECT showed no involvement of the liver or lungs. Following chemoradiation, what is the next best step in management?
Why should acute mechanical large bowel obstruction be operated on early?
Practice by Chapter
Colorectal Anatomy and Physiology
Practice Questions
Diverticular Disease
Practice Questions
Inflammatory Bowel Disease
Practice Questions
Colorectal Polyps
Practice Questions
Colorectal Cancer
Practice Questions
Anorectal Abscess and Fistula
Practice Questions
Hemorrhoids
Practice Questions
Rectal Prolapse
Practice Questions
Fecal Incontinence
Practice Questions
Intestinal Stomas Creation and Management
Practice Questions
Pelvic Floor Disorders
Practice Questions
Enhanced Recovery After Colorectal Surgery
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app