Breast Surgery — MCQs
On this page
Favorable prognosis with > 90% 5 year survival rate for carcinoma breast is seen in which of the following?
Which of the following statements about Patey's mastectomy is incorrect?
Hadfield's operation is performed for which of the following pathology?
Microdochectomy is the treatment for which of the following?
A female patient underwent mastectomy with axillary lymph node dissection for left breast cancer 3 years ago. She subsequently developed chronic lymphedema of the left arm. She now presents with a blue nodule on the left arm. What is the most likely diagnosis?
Which of the following is the PRIMARY hormonal factor that influences the development of benign breast disease?
In which of the following conditions is breast conservation surgery not indicated?
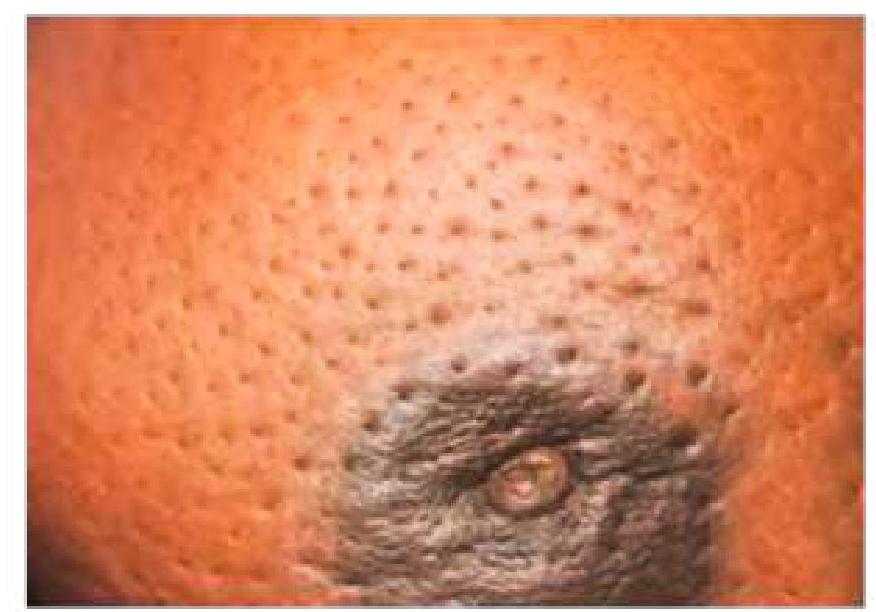
A 59-year-old lady presents with a progressive, painless lump in the breast. What is the cause of the skin change associated with breast cancer?
Which of the following factors is NOT a component of the Van Nuys prognostic index?
Which of the following represents the most definitive guideline-based indication for adjuvant therapy in early breast carcinoma?
Practice by Chapter
Breast Anatomy and Physiology
Practice Questions
Benign Breast Diseases
Practice Questions
Breast Cancer Screening
Practice Questions
Breast Cancer: Diagnosis and Staging
Practice Questions
Surgical Management of Breast Cancer
Practice Questions
Oncoplastic Breast Surgery
Practice Questions
Sentinel Lymph Node Biopsy
Practice Questions
Axillary Surgery
Practice Questions
Breast Reconstruction Techniques
Practice Questions
Male Breast Disorders
Practice Questions
Phyllodes Tumors
Practice Questions
Management of Ductal Carcinoma In Situ
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app