Breast Surgery — MCQs
On this page
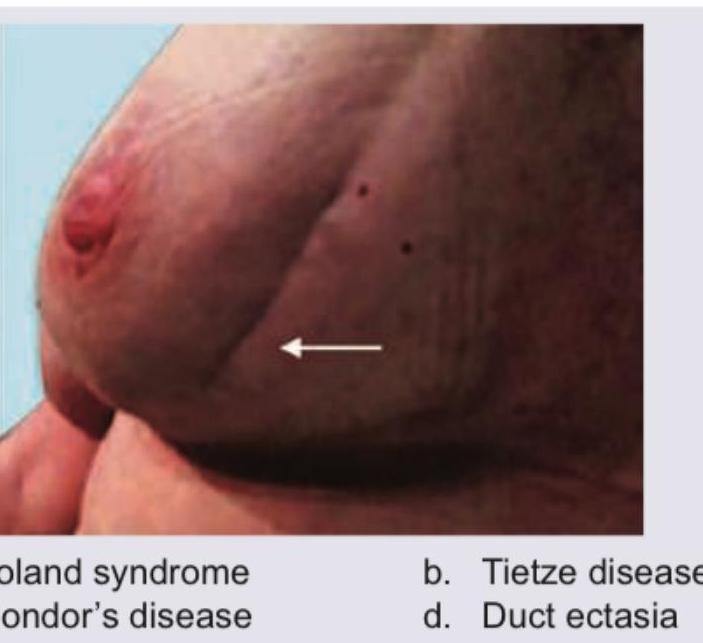
All are true about the condition shown except?

All of the following are true regarding this picture except: (Recent NEET Pattern 2016-17)

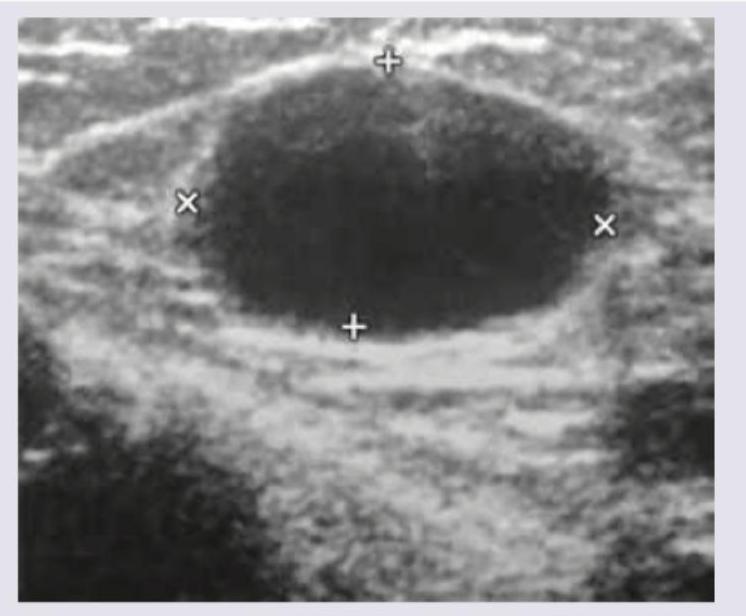
What is the most possible diagnosis?
A 25-year-old woman presents with a painless lump in her right breast that has been gradually enlarging over the past 6 months. On examination, the lump is firm, mobile, and non-tender. USG breast shows a well-defined, hypoechoic, oval solid mass measuring 3.5 cm with smooth margins. FNAC is concordant with fibroadenoma. What is true regarding the management of this condition? (Recent NEET Pattern 2016-17)
A perimenopausal woman presents with chronic multiduct green-brown nipple discharge and the following image. Ultrasound shows subareolar duct dilatation. The diagnosis is:

All are true about the condition shown in the image except:

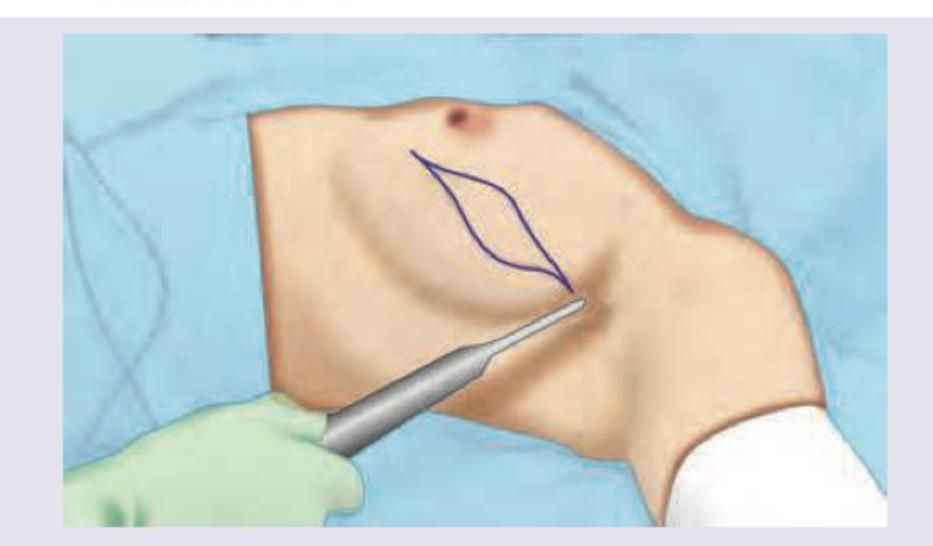
What technique has been depicted in the image shown below?
A 45-year-old lady presents with history of a painless lump in the right breast since 1 month. On examination, the lump is hard, 3 x 4 cm in size in the upper outer quadrant and is not fixed to the skin or the underlying structures. The axilla reveals firm mobile lymph nodes (level I). Rest of systemic examination is normal. The clinical stage of this disease is :
The best cosmetic result following breast reconstruction is achieved with :
Which of the following is the FIRST step in triple assessment of breast lumps? 1. Clinical assessment 2. Radiological assessment 3. Histopathological assessment 4. Sentinel lymph node biopsy
Practice by Chapter
Breast Anatomy and Physiology
Practice Questions
Benign Breast Diseases
Practice Questions
Breast Cancer Screening
Practice Questions
Breast Cancer: Diagnosis and Staging
Practice Questions
Surgical Management of Breast Cancer
Practice Questions
Oncoplastic Breast Surgery
Practice Questions
Sentinel Lymph Node Biopsy
Practice Questions
Axillary Surgery
Practice Questions
Breast Reconstruction Techniques
Practice Questions
Male Breast Disorders
Practice Questions
Phyllodes Tumors
Practice Questions
Management of Ductal Carcinoma In Situ
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app