Breast Surgery — MCQs
On this page
A 36-year-old woman complains of a 3-month history of bloody discharge from the nipple. On examination, a small nodule is found deep to the areola. Careful palpation of the nipple-areolar complex results in blood appearing at the 3 o'clock position. Mammogram findings are normal. What is the likeliest diagnosis?
Conservative surgery is not indicated in breast carcinoma if there is?
A 35-year-old female patient presents with a painless lump in the upper outer quadrant of the right breast noticed 3 months ago. On examination, there is a 2.5 cm firm, irregular, non-tender mass in the upper outer quadrant with no skin changes and no nipple discharge. The nipple-areola complex is clinically uninvolved. Core needle biopsy confirms invasive ductal carcinoma, grade II. Staging workup reveals no distant metastases (T2 N0 M0, Stage IIA). Axillary lymph nodes are clinically negative. The patient has a large breast-to-tumor ratio, no contraindication to surgery, and strongly prefers to avoid breast conservation due to personal preference, requesting the most oncologically appropriate mastectomy option that preserves cosmesis. What is the recommended surgical treatment?
The Van Nuys prognostic index is not based on which of the following parameters?
What is the most frequently used procedure for diagnosing palpable breast masses?
Zuska disease is an eponym for what condition?
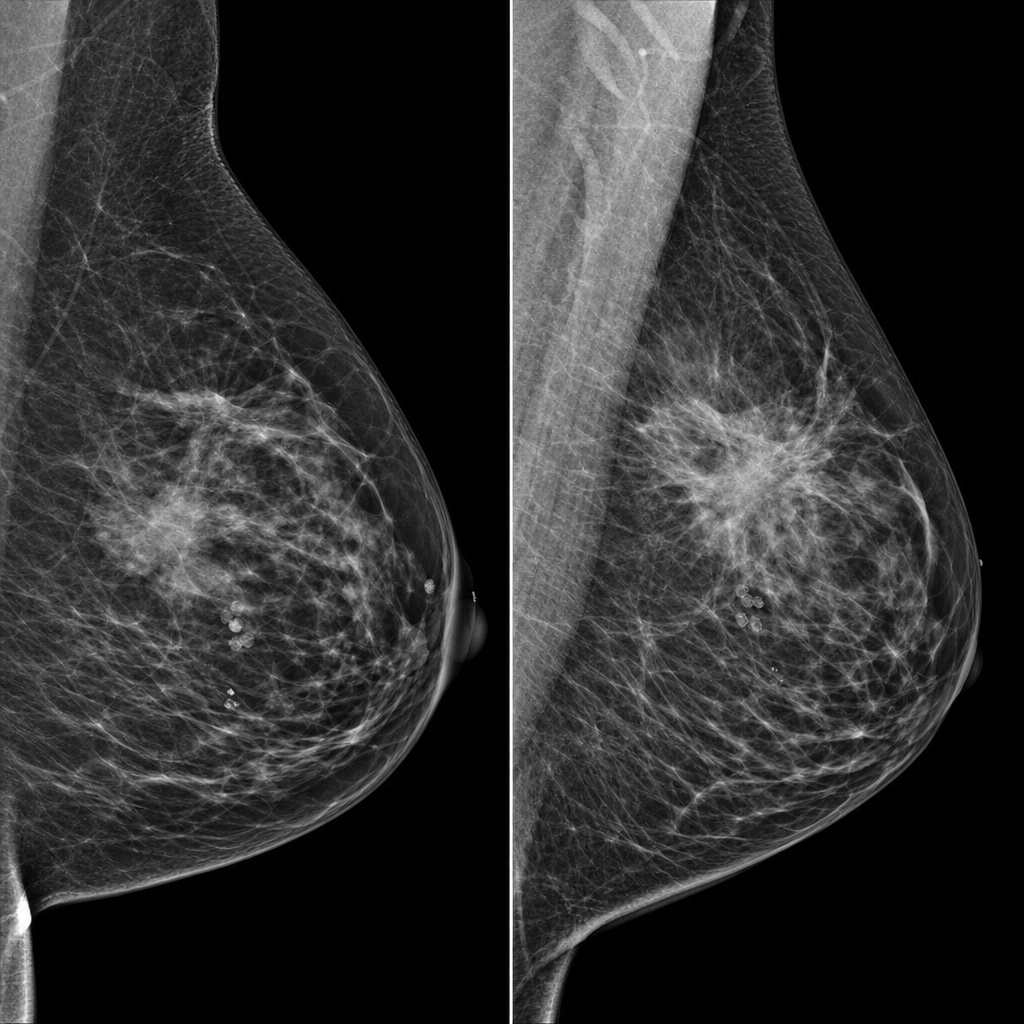
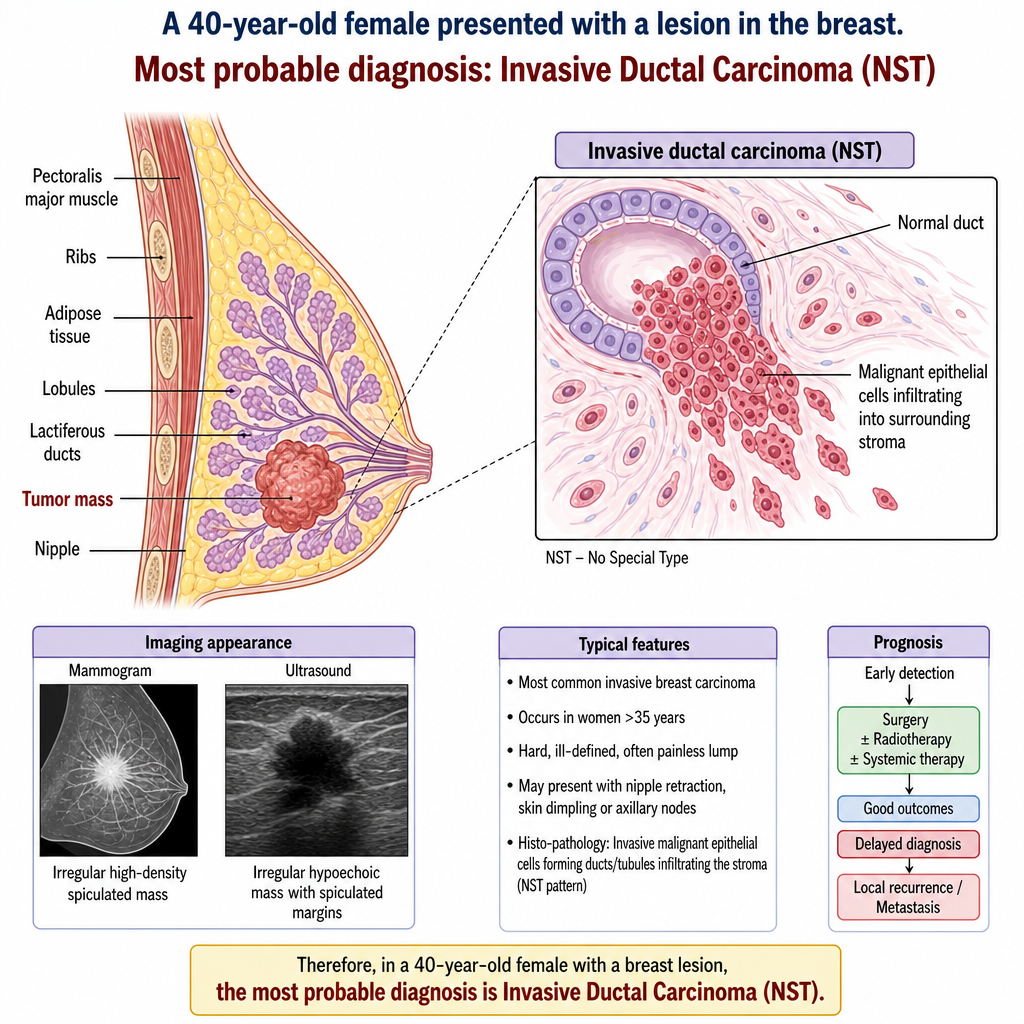
A 40-year-old female presented to the OPD with a lesion in the breast. What is the most probable diagnosis?
A 17-year-old female underwent Fine Needle Aspiration cytology (FNAC) for a lump in the breast which was non-tender, firm and mobile. Which of the following features would suggest a benign breast disease?
Which of the following is not included in the carcinoma in-situ category?
What is the treatment of choice for a duct papilloma of the breast?
Practice by Chapter
Breast Anatomy and Physiology
Practice Questions
Benign Breast Diseases
Practice Questions
Breast Cancer Screening
Practice Questions
Breast Cancer: Diagnosis and Staging
Practice Questions
Surgical Management of Breast Cancer
Practice Questions
Oncoplastic Breast Surgery
Practice Questions
Sentinel Lymph Node Biopsy
Practice Questions
Axillary Surgery
Practice Questions
Breast Reconstruction Techniques
Practice Questions
Male Breast Disorders
Practice Questions
Phyllodes Tumors
Practice Questions
Management of Ductal Carcinoma In Situ
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app