
Ultrasound — MCQs

On this page
In a fetus with Spina bifida, which of the following sign/signs may be seen on ultrasound?
Which one of the following is NOT the strength of ultrasound as a diagnostic modality?
Banana sign is seen in which of the following conditions?
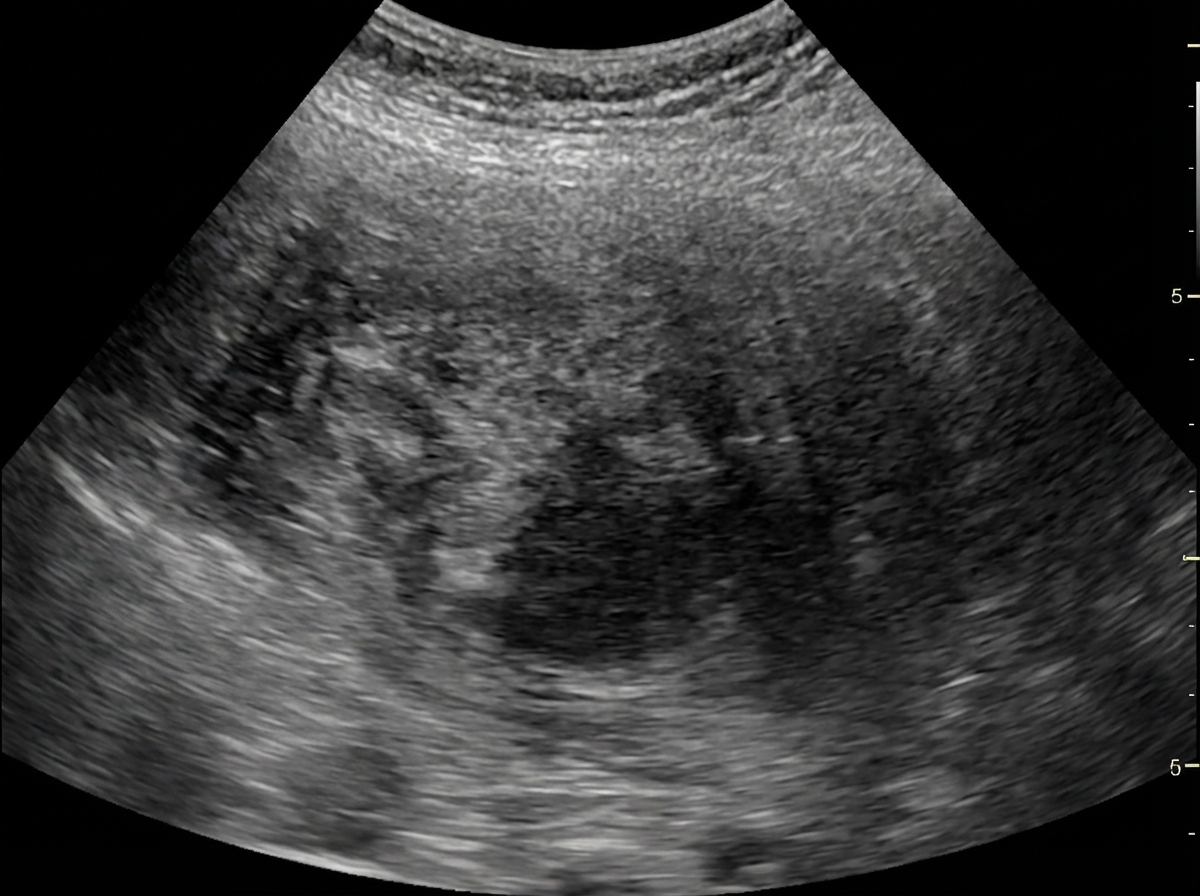
Identify the imaging modality given below.
Which of the following is best assessed by FAST USG?
Red Color on color doppler suggests?
Transrectal ultrasonography in carcinoma prostate is most useful for –
FAST USG focuses on all of the following areas except-
Best method to diagnose hydrocephalus in a fetus at 24 weeks gestation is:
A 40-year-old female was sent to the Radiology department for thyroid USG scan. Which probe will you use for thyroid scan?
Practice by Chapter
Physics of Ultrasound
Practice Questions
Instrumentation and Techniques
Practice Questions
Abdominal Ultrasonography
Practice Questions
Pelvic Ultrasonography
Practice Questions
Obstetric Ultrasonography
Practice Questions
Small Parts Ultrasonography
Practice Questions
Musculoskeletal Ultrasonography
Practice Questions
Vascular Ultrasonography
Practice Questions
Pediatric Ultrasonography
Practice Questions
Contrast-Enhanced Ultrasound
Practice Questions
Ultrasound-Guided Interventions
Practice Questions
Doppler Ultrasound Principles and Applications
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app