
Ultrasound — MCQs

On this page
What is the earliest fetal anomaly detectable by ultrasound?
Which of the following is a primary use of this imaging modality? 
Identify the imaging procedure shown in the image.
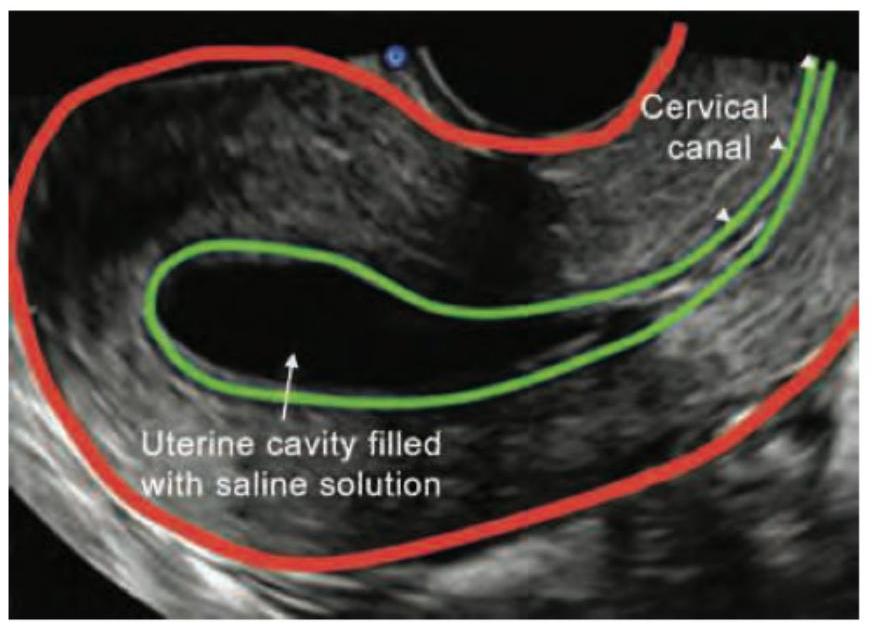
Identify the type of sonography shown:
A pregnant woman undergoes a routine antenatal ultrasound scan in the second trimester. The sonologist notes an abnormal appearance of the fetal cerebellum. What is the sign demonstrated in the given antenatal USG image?

Which one of the following statements is correct regarding eFAST in trauma? 1. It is a technique to assess free fluid in abdominal cavity, thoracic cavity, and pericardium. 2. It is a technique to assess free fluid in pelvic cavity. 3. It is a technique to assess free fluid in pleural cavity. Select the correct answer using the code given below:
"Mickey Mouse Sign" during B-mode duplex ultrasound imaging comprises :
The most difficult area to visualize using duplex scanning (B-mode ultrasound), especially in an obese patient, is
The sonographic finding of a cyst containing clear fluid is described as
Endoluminal probe for transrectal ultrasonography operates at the frequency of:
Practice by Chapter
Physics of Ultrasound
Practice Questions
Instrumentation and Techniques
Practice Questions
Abdominal Ultrasonography
Practice Questions
Pelvic Ultrasonography
Practice Questions
Obstetric Ultrasonography
Practice Questions
Small Parts Ultrasonography
Practice Questions
Musculoskeletal Ultrasonography
Practice Questions
Vascular Ultrasonography
Practice Questions
Pediatric Ultrasonography
Practice Questions
Contrast-Enhanced Ultrasound
Practice Questions
Ultrasound-Guided Interventions
Practice Questions
Doppler Ultrasound Principles and Applications
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app