
Ultrasound — MCQs

On this page
Mercedes Benz sign is seen in:
Following are the ultrasound parameters used in the diagnosis of intrauterine growth restriction except?
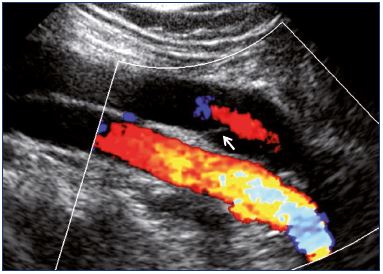
A patient presents with sudden-onset right leg pain. An investigation was done, and the obtained image is shown below. What is the investigation based on the image?
Which of the following is NOT a typical ultrasonographic finding in autosomal recessive polycystic kidney disease (ARPKD)?
Frequency of ultrasound waves in USG -
What is the echogenic lesion size criterion for chronic pancreatitis?
Investigation of choice for screening of proximal internal carotid artery stenosis is :
Which of the following techniques uses piezoelectric crystals?
Which imaging and Doppler techniques are combined in duplex ultrasonography?
What is the best way to diagnose gallbladder stones?
Practice by Chapter
Physics of Ultrasound
Practice Questions
Instrumentation and Techniques
Practice Questions
Abdominal Ultrasonography
Practice Questions
Pelvic Ultrasonography
Practice Questions
Obstetric Ultrasonography
Practice Questions
Small Parts Ultrasonography
Practice Questions
Musculoskeletal Ultrasonography
Practice Questions
Vascular Ultrasonography
Practice Questions
Pediatric Ultrasonography
Practice Questions
Contrast-Enhanced Ultrasound
Practice Questions
Ultrasound-Guided Interventions
Practice Questions
Doppler Ultrasound Principles and Applications
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app