
Ultrasound — MCQs

On this page
What is the earliest fetal anomaly detectable by ultrasound?
Ultrasound scanning of a fetus shows asymmetric growth retardation. It may be associated with which of the following pathologies?
The Sonographic scan given below shows:

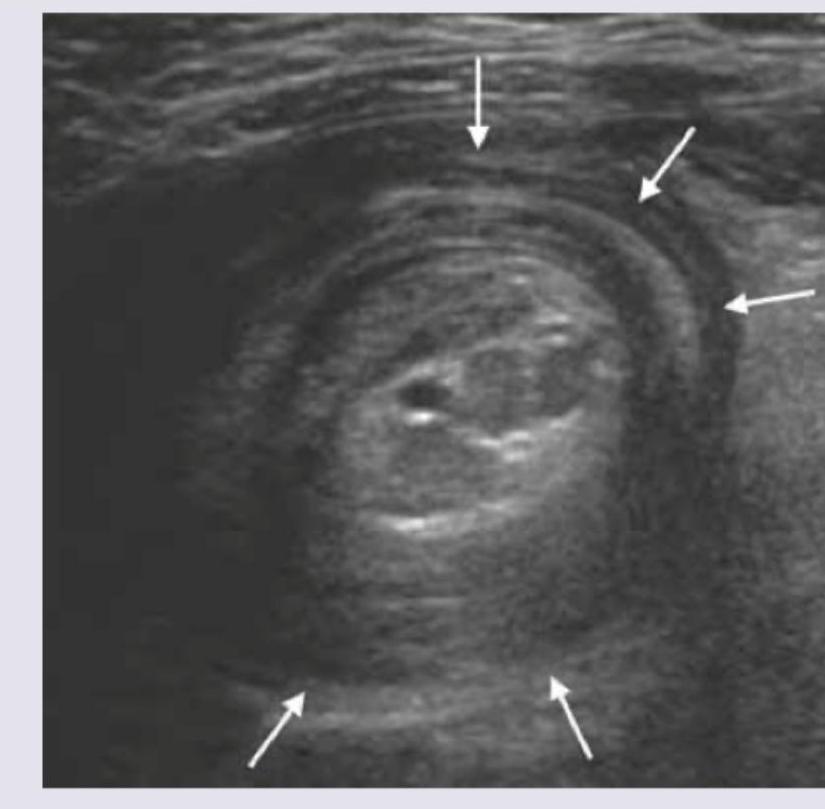
The ultrasound finding of a 7 -month-old child with abdominal pain and mass in the upper abdomen is shown below. What is the diagnosis? (NEET Pattern 2018)
Keyhole sign on fetal ultrasound is seen in:

The first imaging modality of choice for a 35-year-old lady, presenting to surgical emergency with complaints of colicky pain in right lower quadrant of abdomen and vomiting since last 2 days is:
"Mickey Mouse Sign" during B-mode duplex ultrasound imaging comprises :
The most difficult area to visualize using duplex scanning (B-mode ultrasound), especially in an obese patient, is
Foetal anaemia can be detected non-invasively by Doppler ultrasonography on the basis of an increase in the
The sonographic finding of a cyst containing clear fluid is described as
Practice by Chapter
Physics of Ultrasound
Practice Questions
Instrumentation and Techniques
Practice Questions
Abdominal Ultrasonography
Practice Questions
Pelvic Ultrasonography
Practice Questions
Obstetric Ultrasonography
Practice Questions
Small Parts Ultrasonography
Practice Questions
Musculoskeletal Ultrasonography
Practice Questions
Vascular Ultrasonography
Practice Questions
Pediatric Ultrasonography
Practice Questions
Contrast-Enhanced Ultrasound
Practice Questions
Ultrasound-Guided Interventions
Practice Questions
Doppler Ultrasound Principles and Applications
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app