
Ultrasound — MCQs

On this page
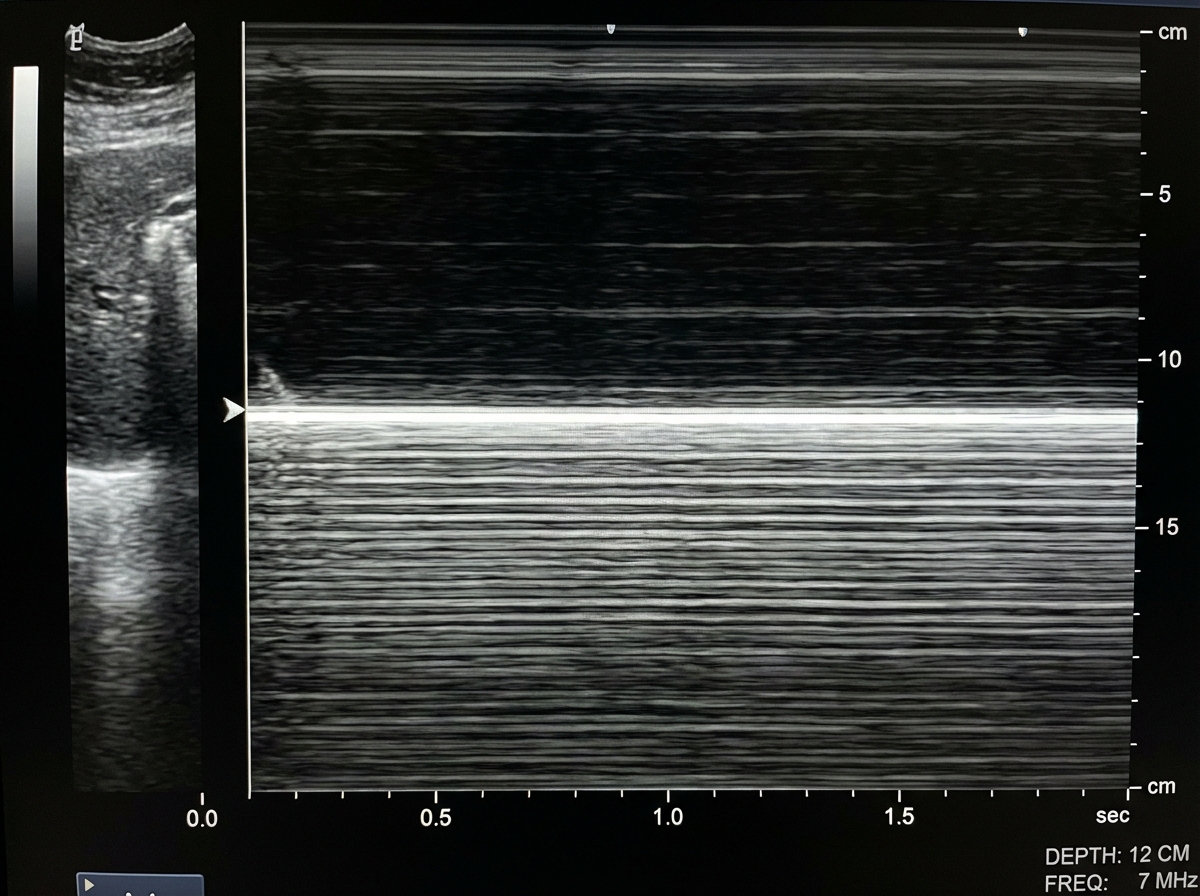
A patient presented with a history of blunt trauma to the chest and abdomen. On USG examination in M mode the following finding is seen. What is the likely diagnosis?
Which of the following is not a prerequisite for transvaginal sonography?
What is the investigation of choice for a lactating female presenting with a painful breast lump?
Nuchal Skin Fold thickness scan is typically performed between which gestational ages?
What is the ideal gestational age for performing ultrasound to assess fetal organ defects?
Distal acoustic shadow is seen in?
What is the investigation of choice to visualize gallbladder pathologies?
All are true about antenatal umbilical artery Doppler except?
Pericardial effusion is best diagnosed by?
What is the initial investigation for an amoebic liver abscess?
Practice by Chapter
Physics of Ultrasound
Practice Questions
Instrumentation and Techniques
Practice Questions
Abdominal Ultrasonography
Practice Questions
Pelvic Ultrasonography
Practice Questions
Obstetric Ultrasonography
Practice Questions
Small Parts Ultrasonography
Practice Questions
Musculoskeletal Ultrasonography
Practice Questions
Vascular Ultrasonography
Practice Questions
Pediatric Ultrasonography
Practice Questions
Contrast-Enhanced Ultrasound
Practice Questions
Ultrasound-Guided Interventions
Practice Questions
Doppler Ultrasound Principles and Applications
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app