
Ultrasound — MCQs

On this page
First line investigation for deep venous thrombosis is -
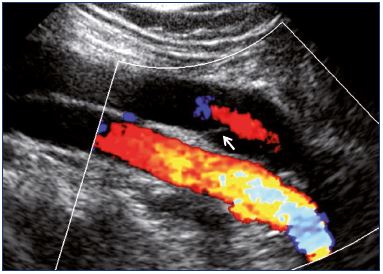
A patient presents with sudden-onset right leg pain. An investigation was done, and the obtained image is shown below. What is the investigation based on the image?
The Doppler effect in medical ultrasound is caused by:
Frequency of ultrasound waves in USG -
Which of the following techniques uses piezoelectric crystals?
Which imaging and Doppler techniques are combined in duplex ultrasonography?
What is the primary advantage of using sector scanning in neonates?
What is the frequency range of ultrasonic sound waves used in medical sonography?
Which of the following structures is LEAST suitable for ultrasound visualization?
Which of the following sonographic findings is most indicative of an intrauterine pregnancy?
Practice by Chapter
Physics of Ultrasound
Practice Questions
Instrumentation and Techniques
Practice Questions
Abdominal Ultrasonography
Practice Questions
Pelvic Ultrasonography
Practice Questions
Obstetric Ultrasonography
Practice Questions
Small Parts Ultrasonography
Practice Questions
Musculoskeletal Ultrasonography
Practice Questions
Vascular Ultrasonography
Practice Questions
Pediatric Ultrasonography
Practice Questions
Contrast-Enhanced Ultrasound
Practice Questions
Ultrasound-Guided Interventions
Practice Questions
Doppler Ultrasound Principles and Applications
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app