
Radiological Anatomy — MCQs

On this page
Normal prevertebral soft tissue thickness in adults at C3 level is
Which of the following is most difficult to locate?
Regarding contrast radiography which among the following is FALSE?
McGregor line and Chamberlain's line are seen in?
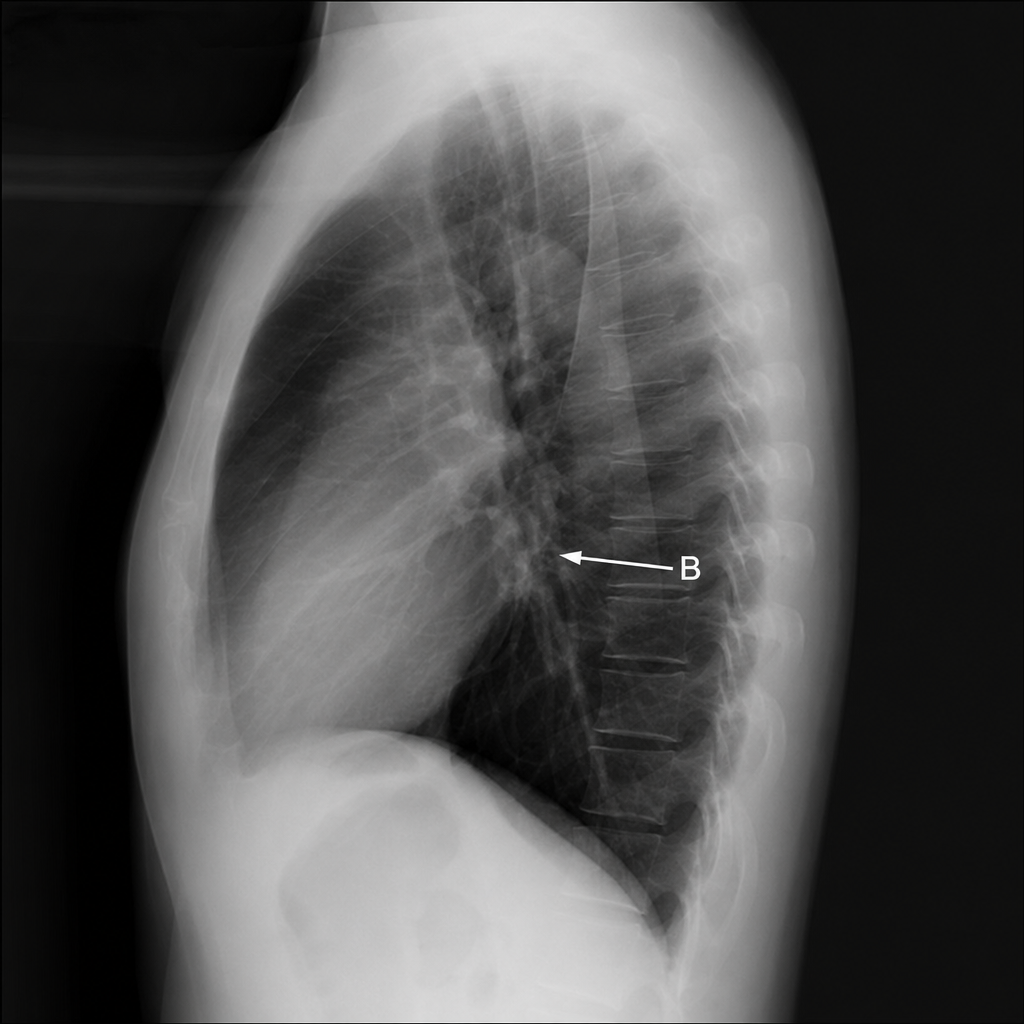
What is the structure 'B' marked in lateral chest X-ray below?
Radiological view which best shows maxillary sinus and orbit is -
Which radiographic view is best for visualizing the sphenoid sinus?
Water’s view is used to obtain diagnostic information of:
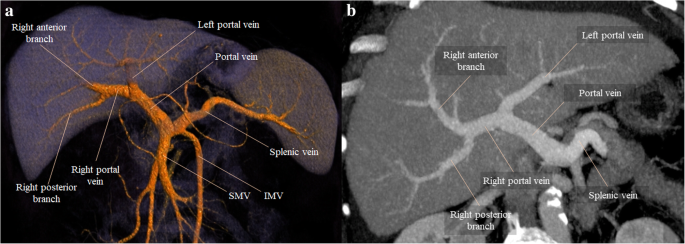
Identify the structure branching into the liver as seen in the provided CT scan of the abdomen.
Caldwell’s view is primarily used to visualize which sinus?
Practice by Chapter
Radiographic Anatomy of Skull and Face
Practice Questions
Radiographic Anatomy of Spine
Practice Questions
Radiographic Anatomy of Chest
Practice Questions
Radiographic Anatomy of Abdomen
Practice Questions
Radiographic Anatomy of Extremities
Practice Questions
Cross-sectional Anatomy: Brain and Head
Practice Questions
Cross-sectional Anatomy: Neck
Practice Questions
Cross-sectional Anatomy: Thorax
Practice Questions
Cross-sectional Anatomy: Abdomen and Pelvis
Practice Questions
Vascular Anatomy
Practice Questions
Developmental Anatomy Variations
Practice Questions
Anatomic Landmarks for Interventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app