
Radiological Anatomy — MCQs

On this page
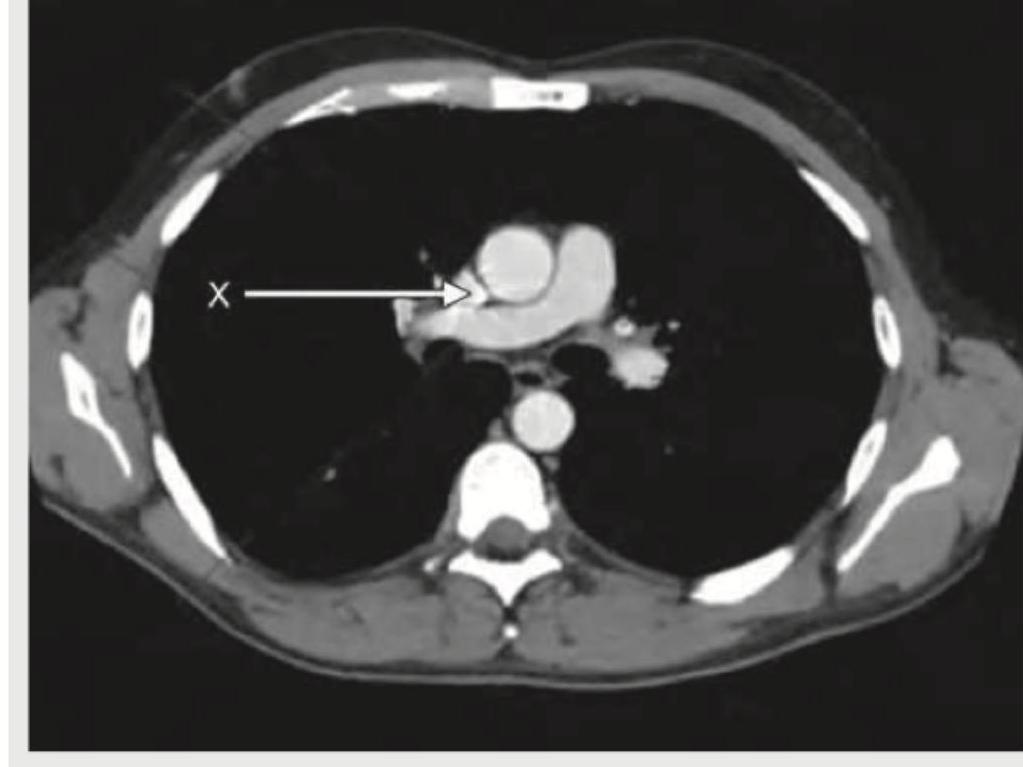
The X mark in the following CT chest shows:
The lateral view chest X-ray shows:

Identify the structure shown in CT abdomen section. (Recent NEET Pattern 2018-19)
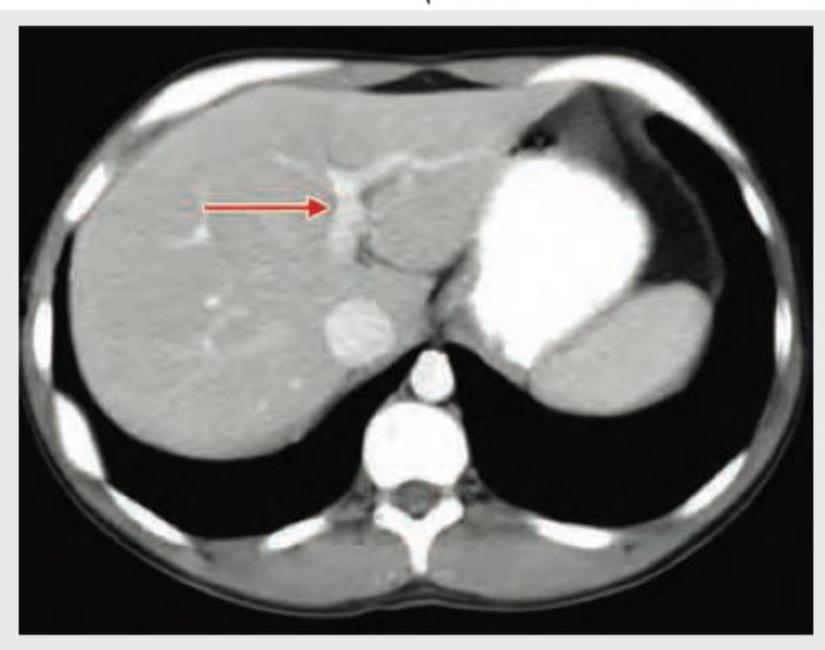
Identify the marked structure in the CT abdomen section shown below? (Recent NEET Pattern 2018-19)

A 25-year-old female presents with neck pain and tingling sensation in her left arm. An X-ray of the cervicothoracic region is obtained. What is the radiological finding shown in the image?

Radiologic views used for fracture Mandible (body and Ramus) are all EXCEPT:
The perorbital view is carried out for -
The Transorbital view is carried out for:
Which term describes the internal appearance of a lesion?
The best view to visualize zygomatic arches is
Practice by Chapter
Radiographic Anatomy of Skull and Face
Practice Questions
Radiographic Anatomy of Spine
Practice Questions
Radiographic Anatomy of Chest
Practice Questions
Radiographic Anatomy of Abdomen
Practice Questions
Radiographic Anatomy of Extremities
Practice Questions
Cross-sectional Anatomy: Brain and Head
Practice Questions
Cross-sectional Anatomy: Neck
Practice Questions
Cross-sectional Anatomy: Thorax
Practice Questions
Cross-sectional Anatomy: Abdomen and Pelvis
Practice Questions
Vascular Anatomy
Practice Questions
Developmental Anatomy Variations
Practice Questions
Anatomic Landmarks for Interventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app