
Radiological Anatomy — MCQs

On this page
A radiograph of a 32-year-old patient reveals an asymptomatic lesion that was an accidental finding. What is the most likely diagnosis?

A patient with a history of trauma presents with hearing loss. A High-Resolution Computed Tomography (HRCT) scan was performed. Which of the following structures is not typically visualized on HRCT?
Identify the part of the bowel in the barium study given below.
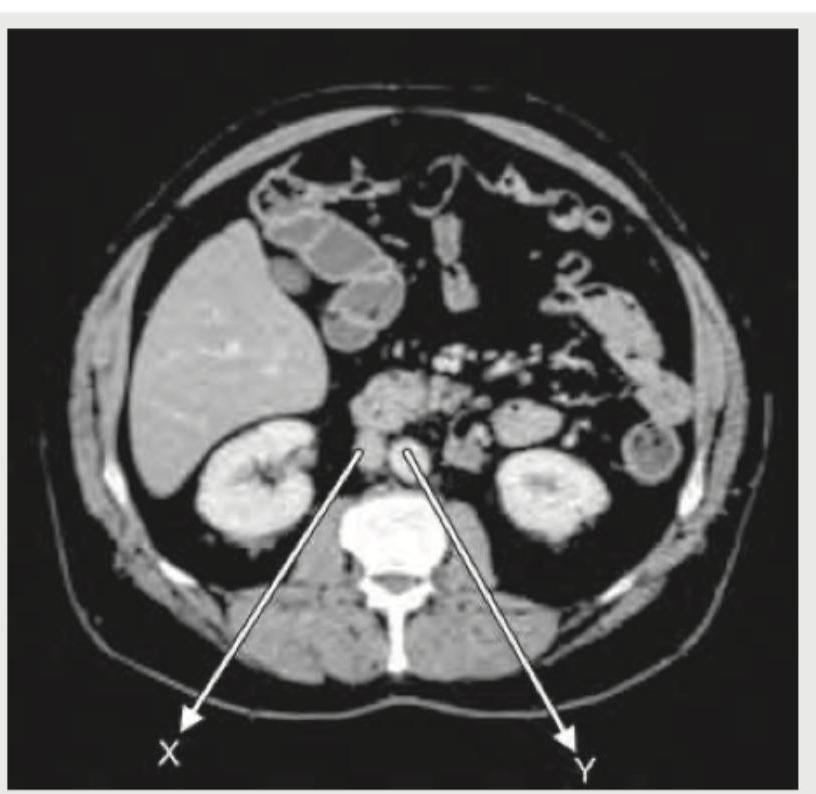
The structure marked by arrow in CT abdomen:

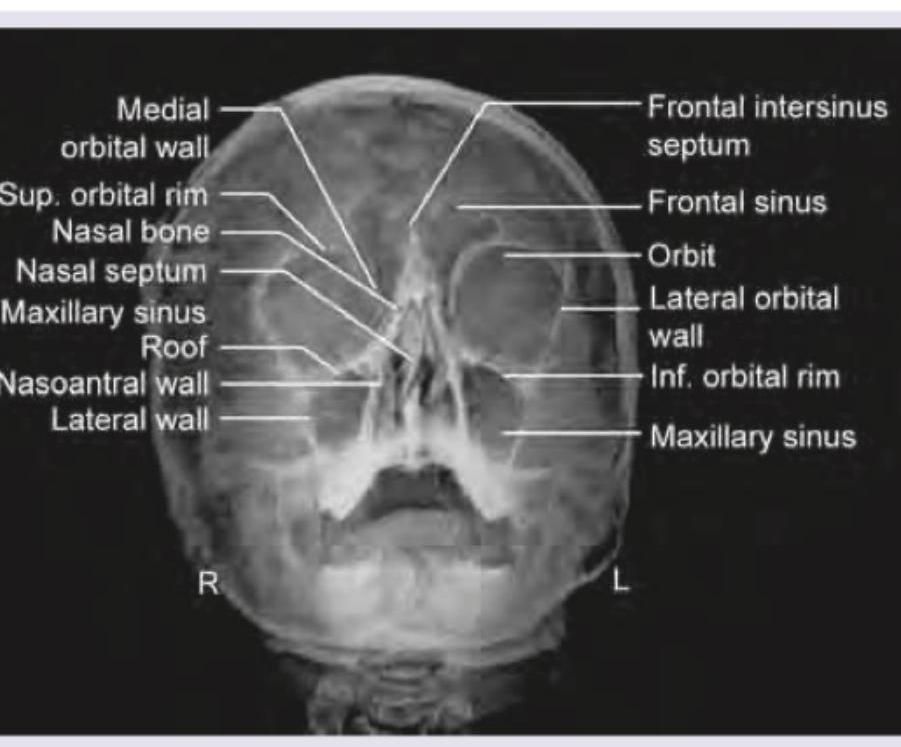
The given X-ray of paranasal sinuses shows which view?
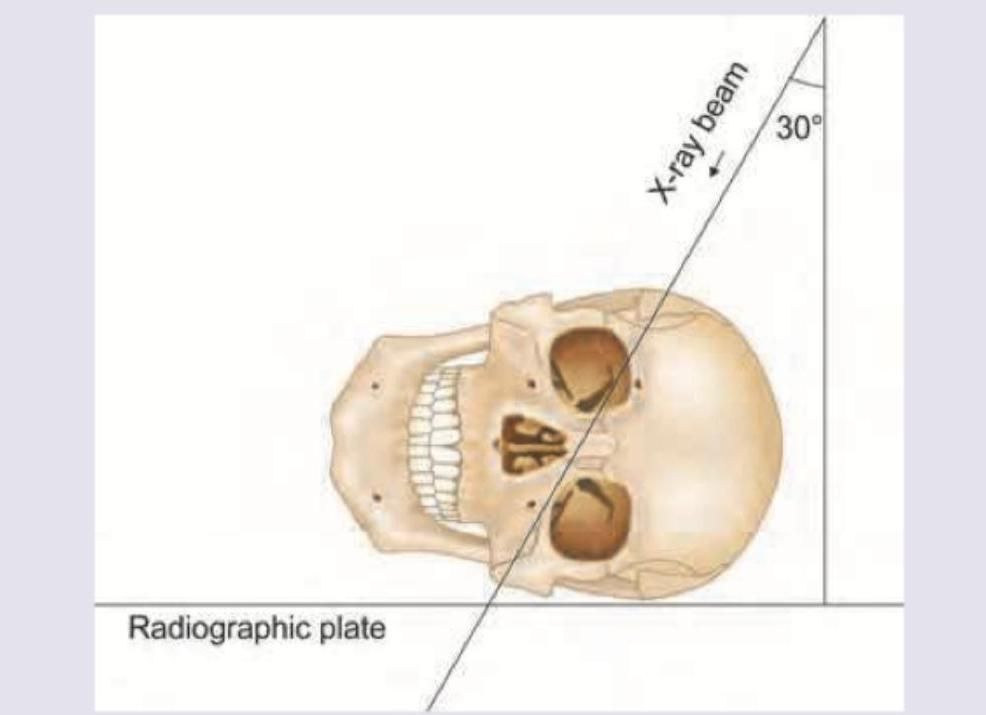
A radiographic projection with X-ray beam angled at 30 degrees to the radiographic plate, with the skull positioned laterally (as shown in the image), is used to visualize which of the following structures?
The following X-ray is used to evaluate \qquad sinus?
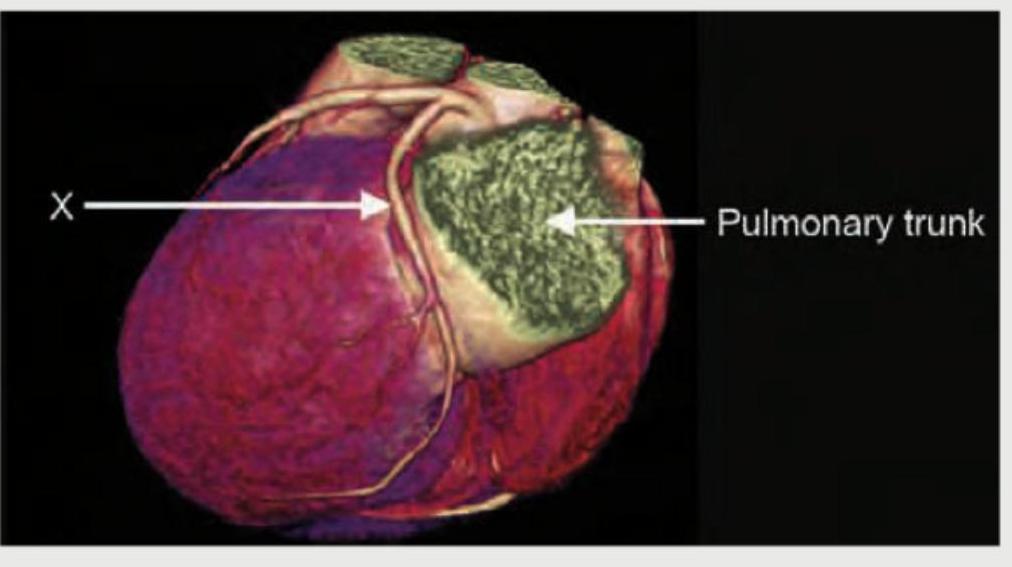
What is the name of the marked blood vessel shown in the CT coronary angiography image?
Which is correct about the CT abdomen shown?
The following CT abdomen shows:

Practice by Chapter
Radiographic Anatomy of Skull and Face
Practice Questions
Radiographic Anatomy of Spine
Practice Questions
Radiographic Anatomy of Chest
Practice Questions
Radiographic Anatomy of Abdomen
Practice Questions
Radiographic Anatomy of Extremities
Practice Questions
Cross-sectional Anatomy: Brain and Head
Practice Questions
Cross-sectional Anatomy: Neck
Practice Questions
Cross-sectional Anatomy: Thorax
Practice Questions
Cross-sectional Anatomy: Abdomen and Pelvis
Practice Questions
Vascular Anatomy
Practice Questions
Developmental Anatomy Variations
Practice Questions
Anatomic Landmarks for Interventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app