
Radiological Anatomy — MCQs

On this page
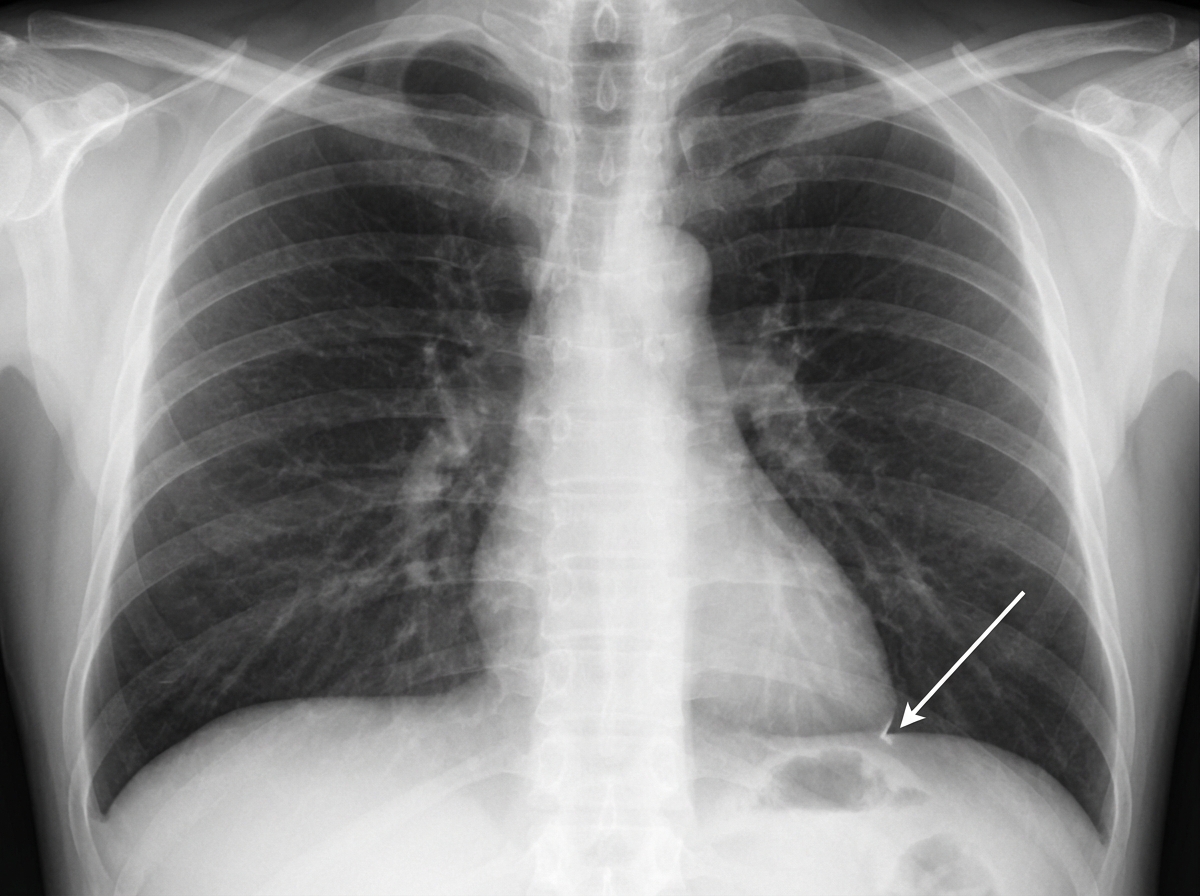
Identify the structure indicated in the given chest X-ray.
At 1 year of age, how many carpal bones are typically visible on a skiagram of the hand?
'Towne's view' in X-ray is used for visualizing which of the following structures?
Shenton line is a radiological landmark seen in which joint on X-ray?
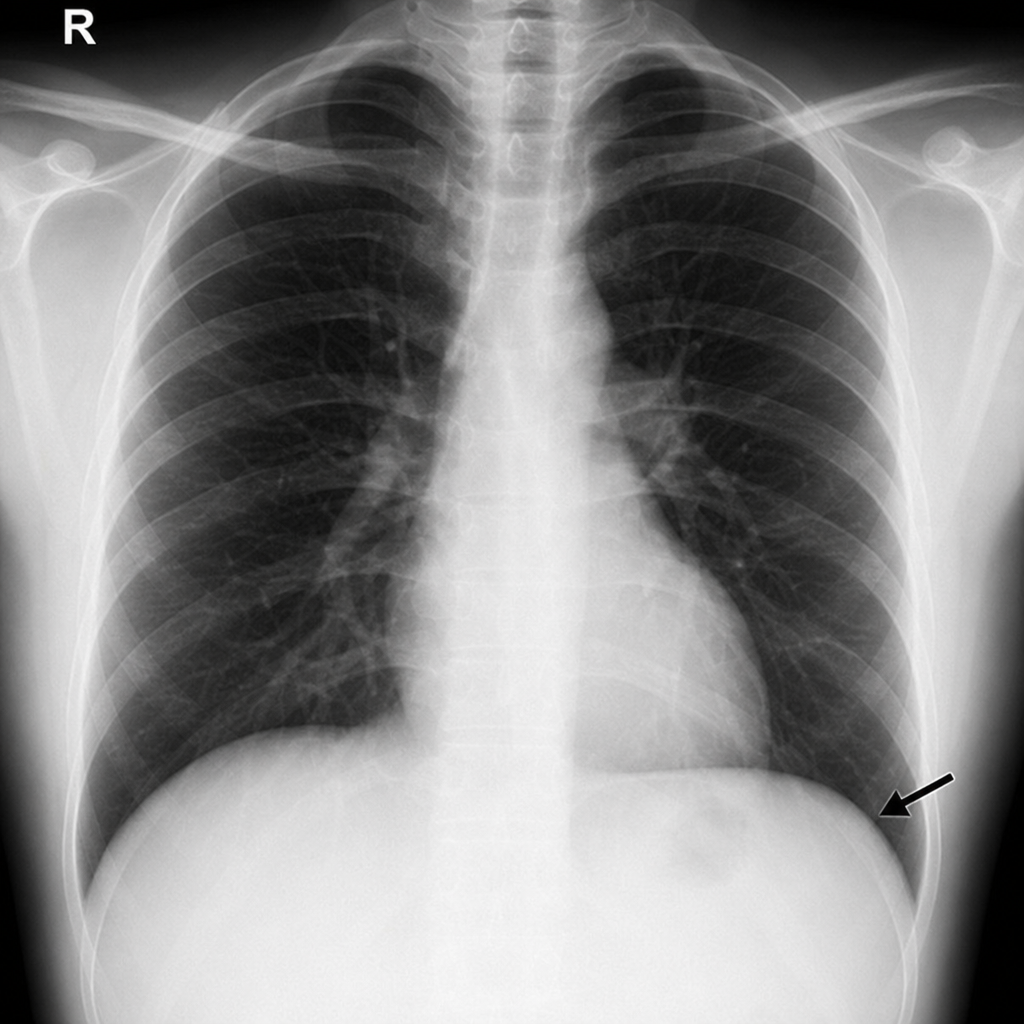
The arrow is pointing to which of the following structures?
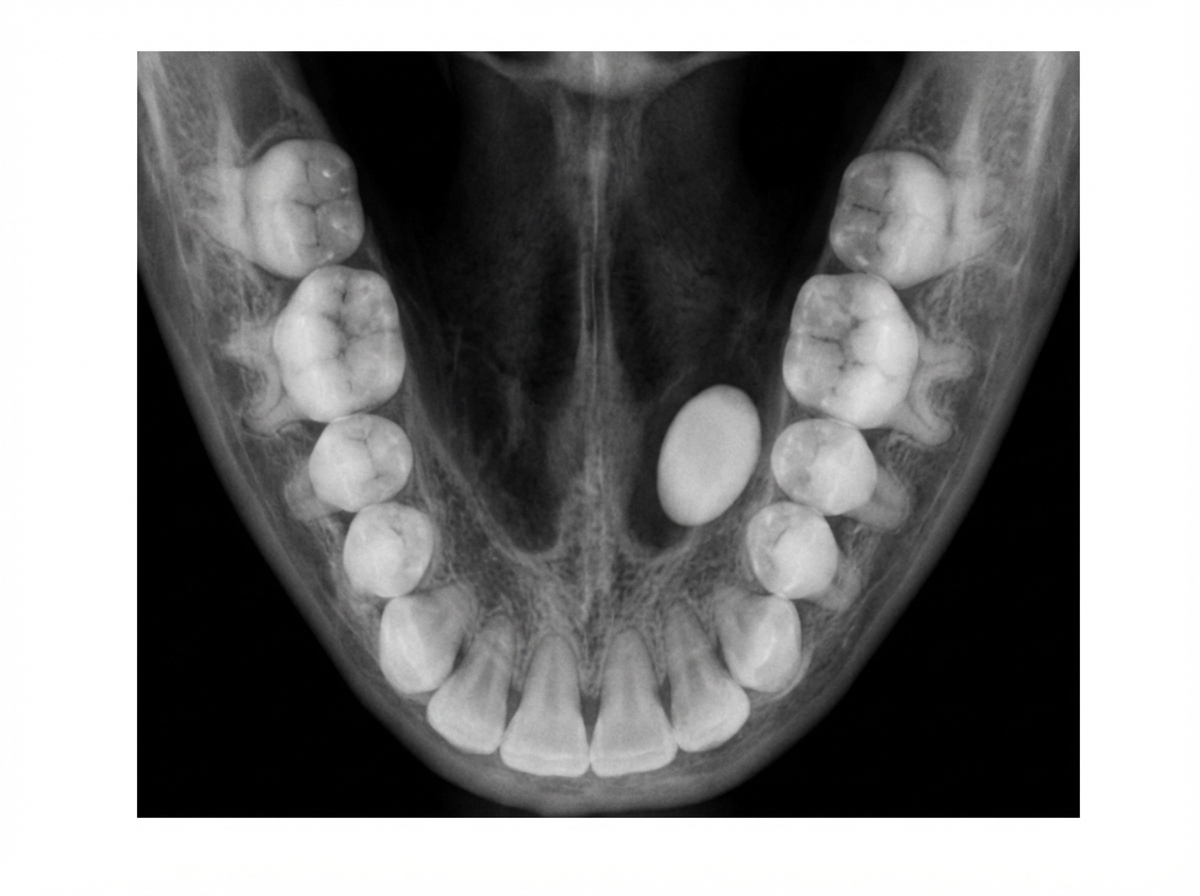
The following occlusal radiograph shows:
Which bones ossify at birth?
Which of the following structures is not visualized on a coronal CT scan of the paranasal sinuses?
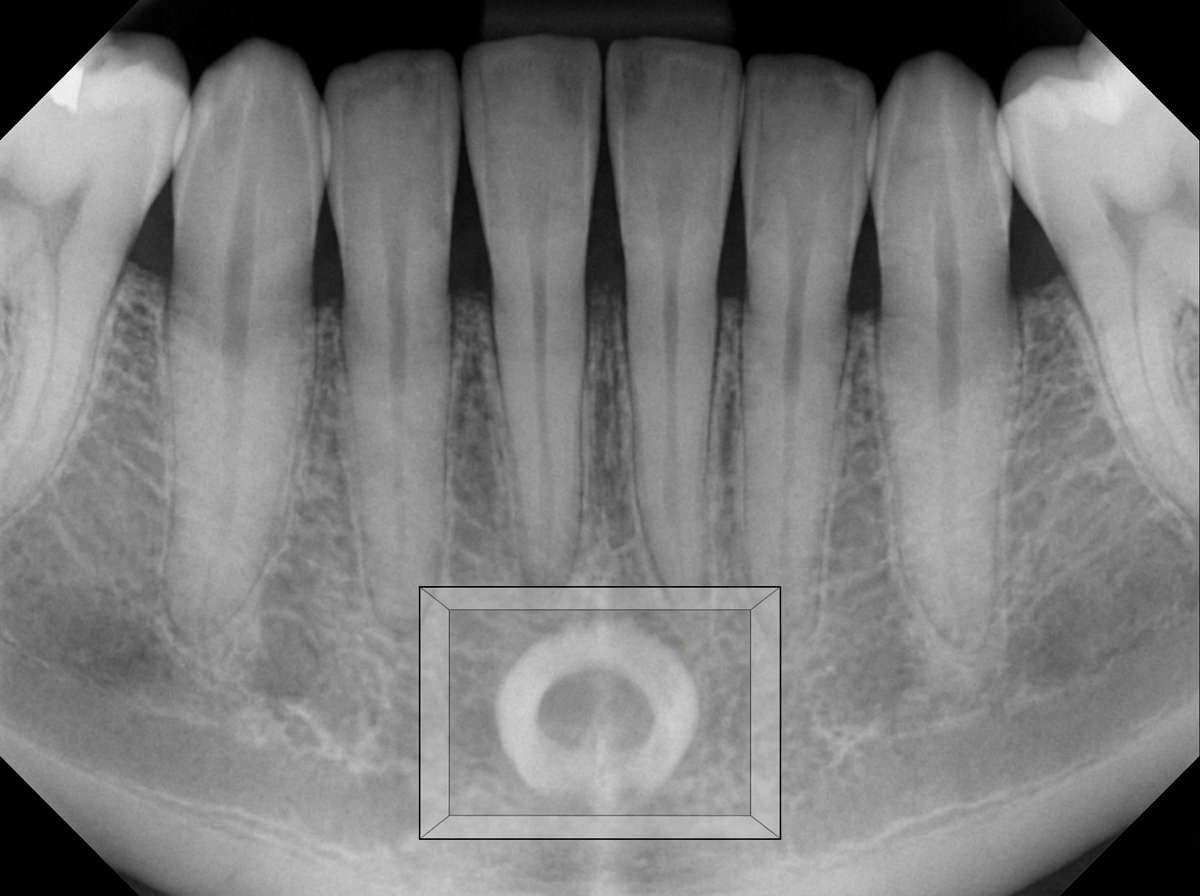
The radiopaque ring (not the central radiolucency) shown in the box is most likely:
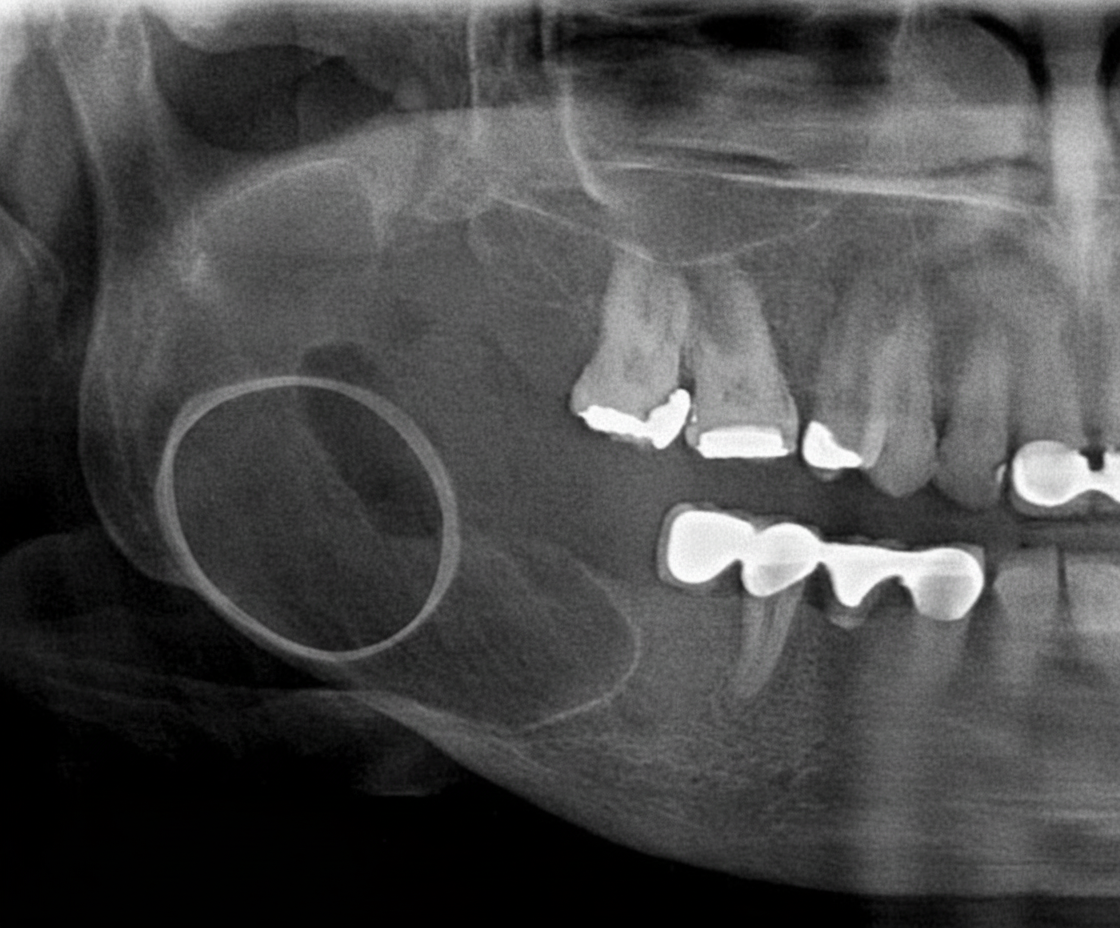
A radiograph of a 32-year-old patient reveals an asymptomatic lesion that was an accidental finding. What is the most likely diagnosis?
Practice by Chapter
Radiographic Anatomy of Skull and Face
Practice Questions
Radiographic Anatomy of Spine
Practice Questions
Radiographic Anatomy of Chest
Practice Questions
Radiographic Anatomy of Abdomen
Practice Questions
Radiographic Anatomy of Extremities
Practice Questions
Cross-sectional Anatomy: Brain and Head
Practice Questions
Cross-sectional Anatomy: Neck
Practice Questions
Cross-sectional Anatomy: Thorax
Practice Questions
Cross-sectional Anatomy: Abdomen and Pelvis
Practice Questions
Vascular Anatomy
Practice Questions
Developmental Anatomy Variations
Practice Questions
Anatomic Landmarks for Interventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app