
Radiological Anatomy — MCQs

On this page
In which condition is the Lambda-Panda sign typically observed?
Christmas tree appearance of urinary bladder is seen in
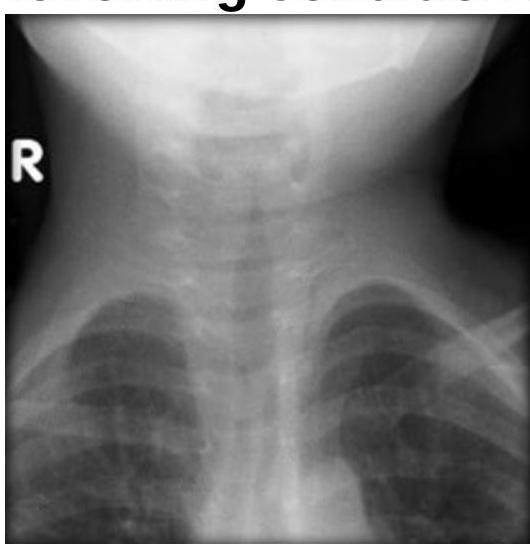
Steeple sign is seen in which of the following conditions?
Which of the following statements about lipoma is radiologically true?
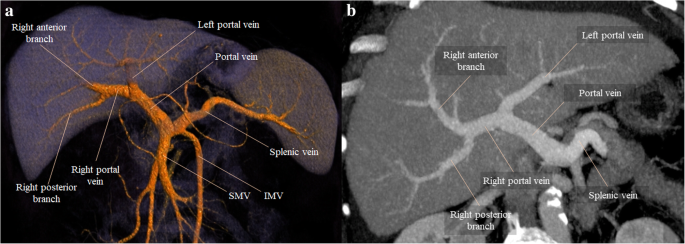
Identify the structure branching into the liver as seen in the provided CT scan of the abdomen.
Water’s view is used to obtain diagnostic information of:
Caldwell’s view is primarily used to visualize which sinus?
Which of the following statements about MRI is incorrect?
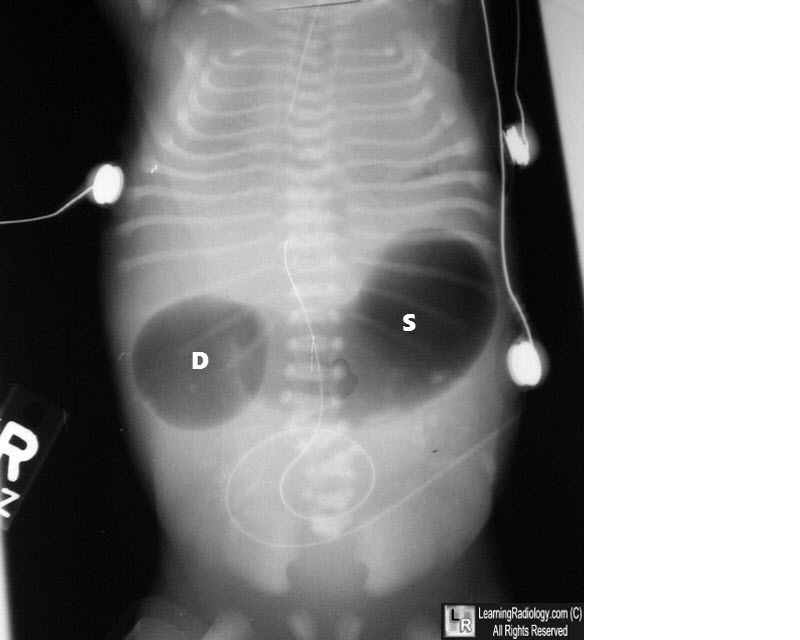
What condition is indicated by the double bubble sign on an abdominal X-ray?
What is the primary use of the Rhese view in radiographic imaging?
Practice by Chapter
Radiographic Anatomy of Skull and Face
Practice Questions
Radiographic Anatomy of Spine
Practice Questions
Radiographic Anatomy of Chest
Practice Questions
Radiographic Anatomy of Abdomen
Practice Questions
Radiographic Anatomy of Extremities
Practice Questions
Cross-sectional Anatomy: Brain and Head
Practice Questions
Cross-sectional Anatomy: Neck
Practice Questions
Cross-sectional Anatomy: Thorax
Practice Questions
Cross-sectional Anatomy: Abdomen and Pelvis
Practice Questions
Vascular Anatomy
Practice Questions
Developmental Anatomy Variations
Practice Questions
Anatomic Landmarks for Interventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app