
Radiological Anatomy — MCQs

On this page
The prominent left border of the heart is formed by all the following except:
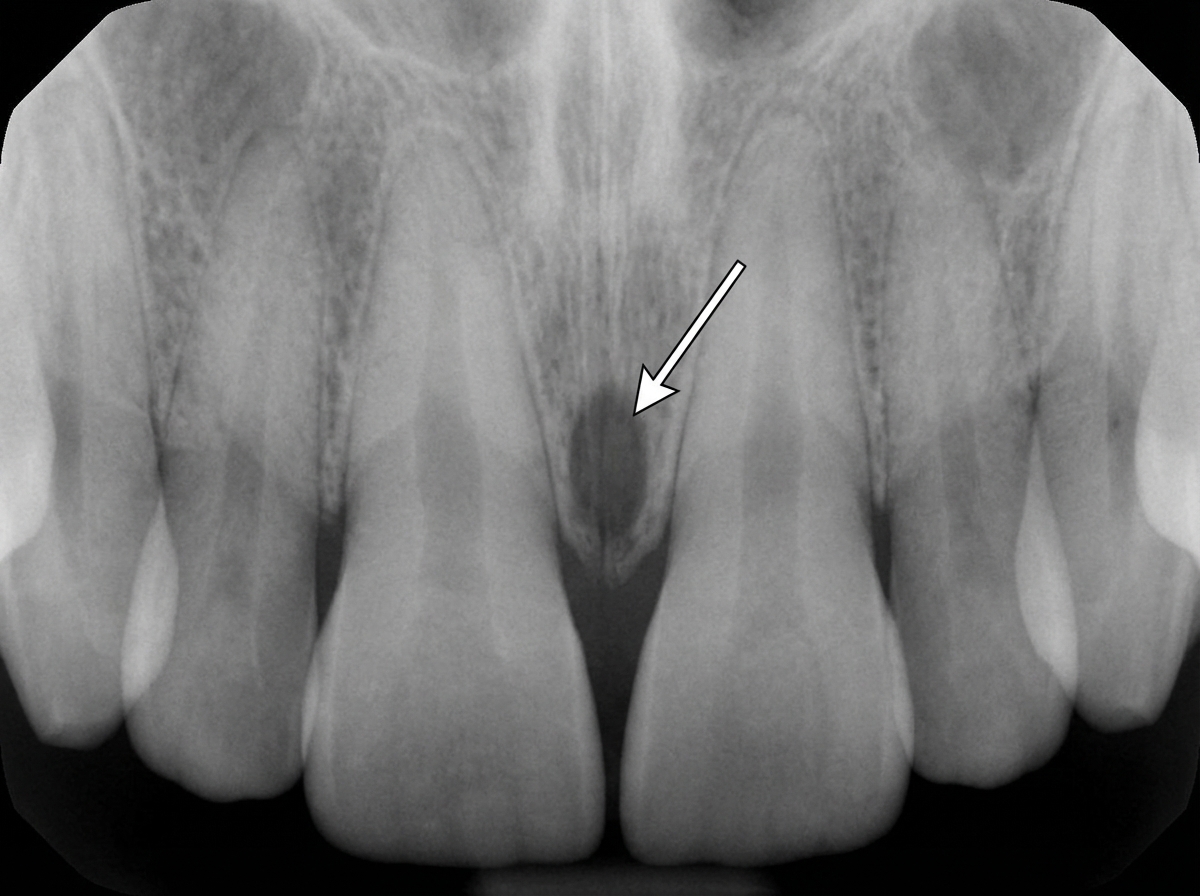
The structure marked with arrows is:
Hilar markings in a normal chest X-ray are formed by all of the following except:
Waters view is best used for visualization of which sinus?
Which anatomical structure is best visualized on a periorbital view X-ray?
Which projection allows for viewing gross osseous changes from a lateral aspect?
Which of the following cranial nerves can be visualized on a plain CT scan?
Zygoma fractures are best visualized on which radiographic view?
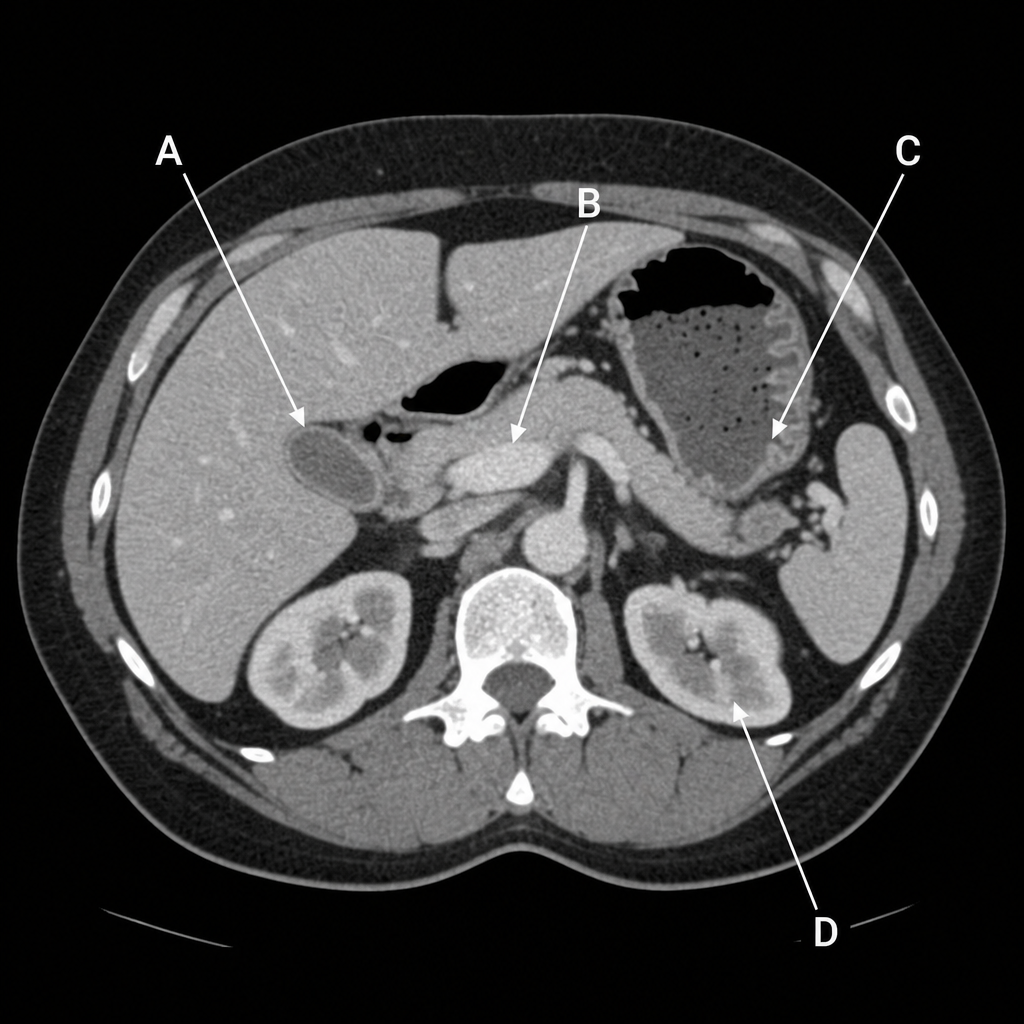
Which structure, as shown in this CT scan of the abdomen at the level of the upper lumbar vertebra, receives bile, concentrates it by absorbing water and salt, and stores it?
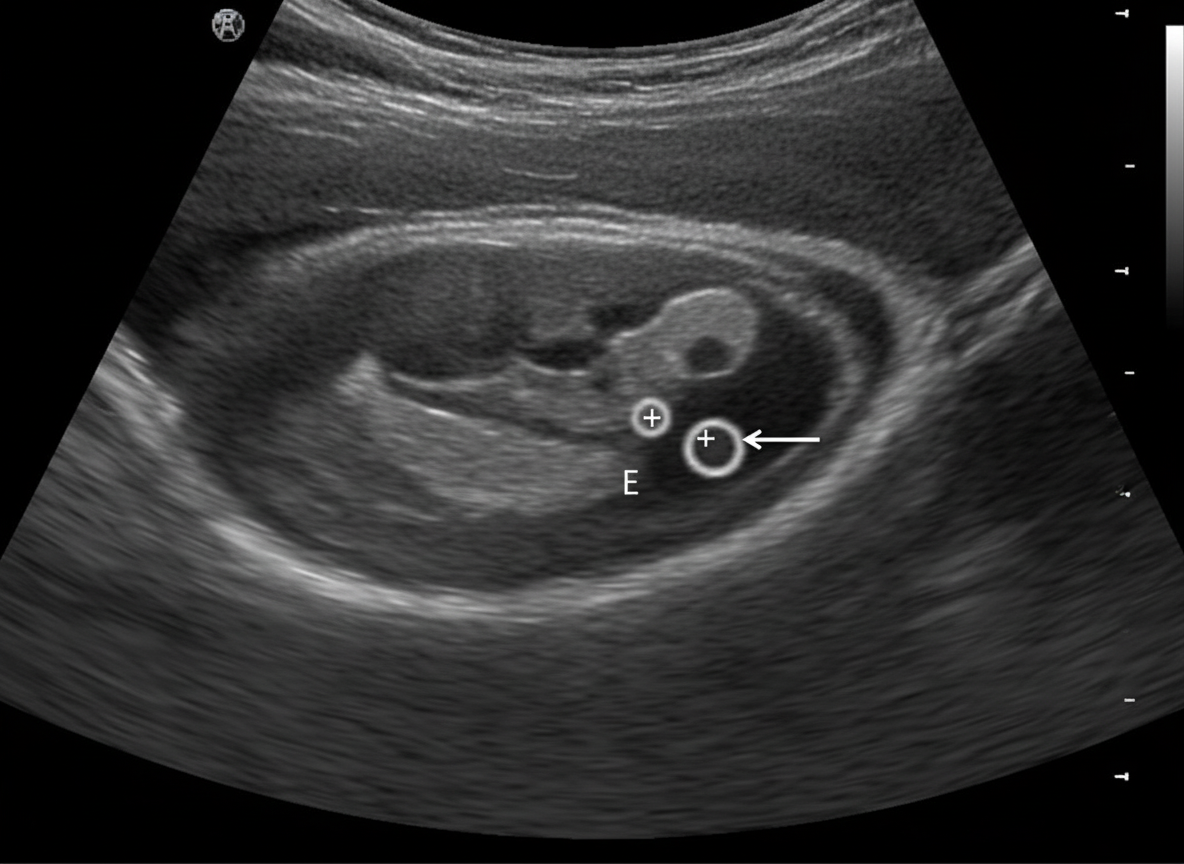
A sonogram demonstrates a Crown-Rump Length (CRL) of an 8-week fetus. The arrow in the image points to which of the following structures?
Practice by Chapter
Radiographic Anatomy of Skull and Face
Practice Questions
Radiographic Anatomy of Spine
Practice Questions
Radiographic Anatomy of Chest
Practice Questions
Radiographic Anatomy of Abdomen
Practice Questions
Radiographic Anatomy of Extremities
Practice Questions
Cross-sectional Anatomy: Brain and Head
Practice Questions
Cross-sectional Anatomy: Neck
Practice Questions
Cross-sectional Anatomy: Thorax
Practice Questions
Cross-sectional Anatomy: Abdomen and Pelvis
Practice Questions
Vascular Anatomy
Practice Questions
Developmental Anatomy Variations
Practice Questions
Anatomic Landmarks for Interventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app