
Radiological Anatomy — MCQs

On this page
Which of the following is the best initial imaging study for evaluating a suspected fracture?
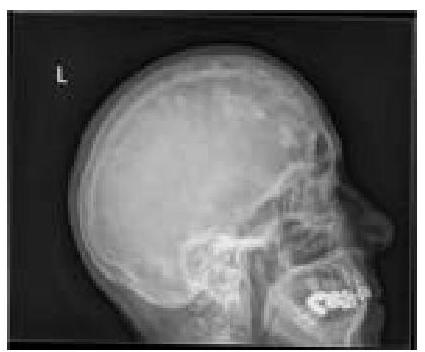
What type of lesions in the skull calvarium can be identified on this X-ray?
Stenver's view is used for -
What is the diagnosis based on the following X-ray?

Which of the following provides excellent details about the chemodectomas?
In normal X-ray of shoulder, which is the superior most structure?
Which radiographic view is best for visualizing the sphenoid sinus?
Radiological view which best shows maxillary sinus and orbit is -
At what age are the first four carpal bones (capitate, hamate, triquetrum, and lunate) typically visible on an X-ray?
Which substance has the highest Hounsfield Unit (HU) value?
Practice by Chapter
Radiographic Anatomy of Skull and Face
Practice Questions
Radiographic Anatomy of Spine
Practice Questions
Radiographic Anatomy of Chest
Practice Questions
Radiographic Anatomy of Abdomen
Practice Questions
Radiographic Anatomy of Extremities
Practice Questions
Cross-sectional Anatomy: Brain and Head
Practice Questions
Cross-sectional Anatomy: Neck
Practice Questions
Cross-sectional Anatomy: Thorax
Practice Questions
Cross-sectional Anatomy: Abdomen and Pelvis
Practice Questions
Vascular Anatomy
Practice Questions
Developmental Anatomy Variations
Practice Questions
Anatomic Landmarks for Interventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app