
Radiological Anatomy — MCQs

On this page
Which of the following structures is best visualised using Schuller's view and Law's view?
Transverse and vertical study of the skeleton can be done in?
"Hair on End" appearance is seen in:
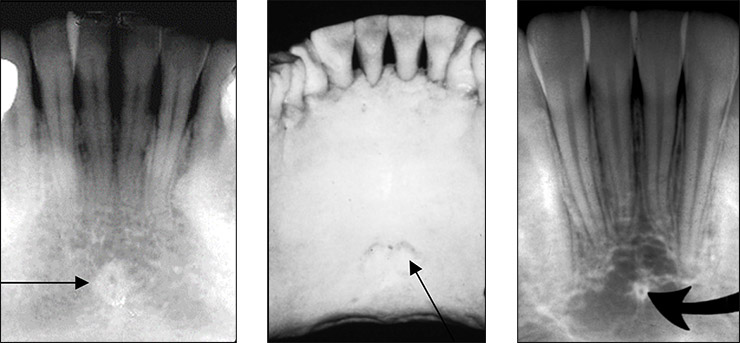
The radiopaque structure shown in the box is most likely:
Which of these structures appears radiopaque?
Which of the following is most radiolucent?
Preferred imaging modality for choanal atresia is
In pantomogram positioning, which anatomical landmark is used for initial patient alignment?
Best view for visualizing sella turcica on X-Ray:
Which of the following will cause posterior impression on barium swallow:
Practice by Chapter
Radiographic Anatomy of Skull and Face
Practice Questions
Radiographic Anatomy of Spine
Practice Questions
Radiographic Anatomy of Chest
Practice Questions
Radiographic Anatomy of Abdomen
Practice Questions
Radiographic Anatomy of Extremities
Practice Questions
Cross-sectional Anatomy: Brain and Head
Practice Questions
Cross-sectional Anatomy: Neck
Practice Questions
Cross-sectional Anatomy: Thorax
Practice Questions
Cross-sectional Anatomy: Abdomen and Pelvis
Practice Questions
Vascular Anatomy
Practice Questions
Developmental Anatomy Variations
Practice Questions
Anatomic Landmarks for Interventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app