
Radiological Anatomy — MCQs

On this page
Multiple radioopacities are seen in which of the following conditions?
A 56-year old man presented with bony pain. What is the most likely diagnosis given an X-ray skull lateral view showing findings consistent with hyperostosis frontalis interna?
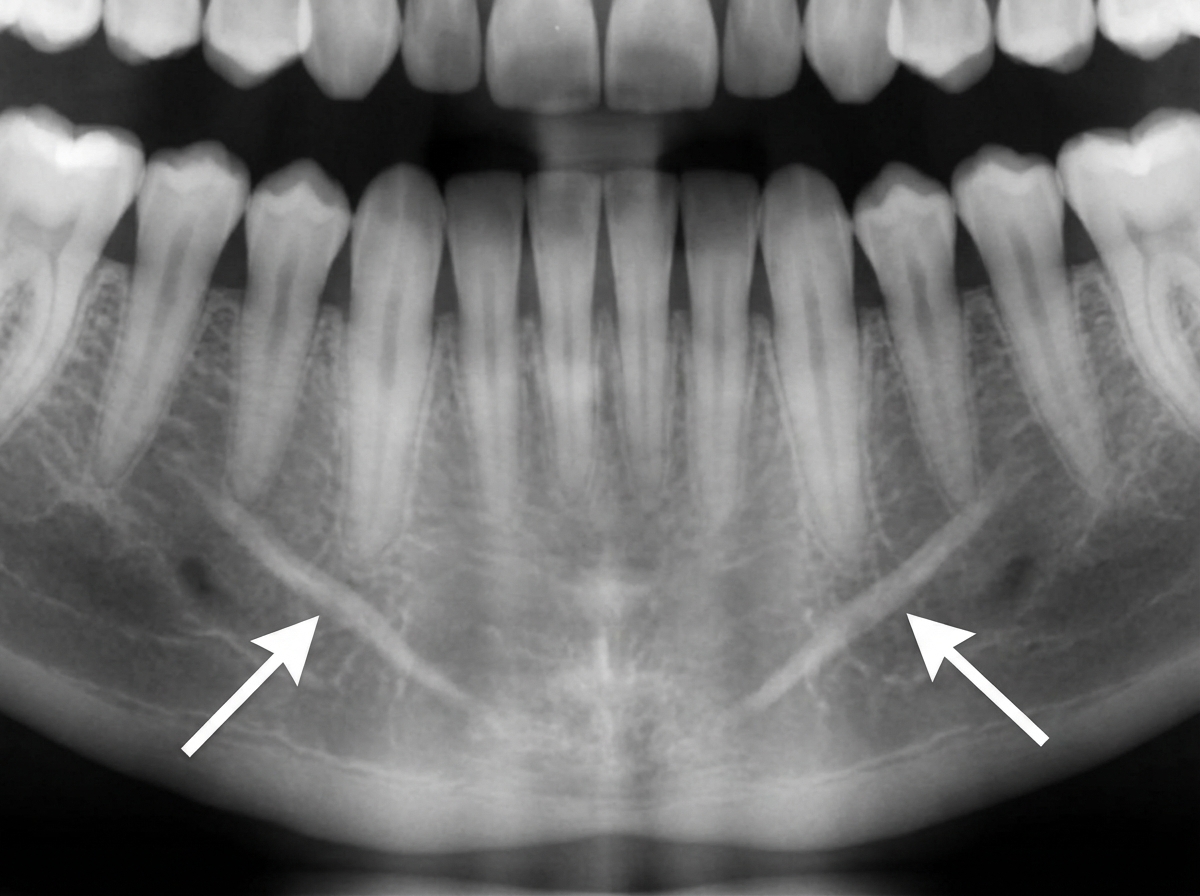
The symmetrical radiopacities marked with arrows are most likely?
Which of the following will appear radiopaque in an X-ray except?
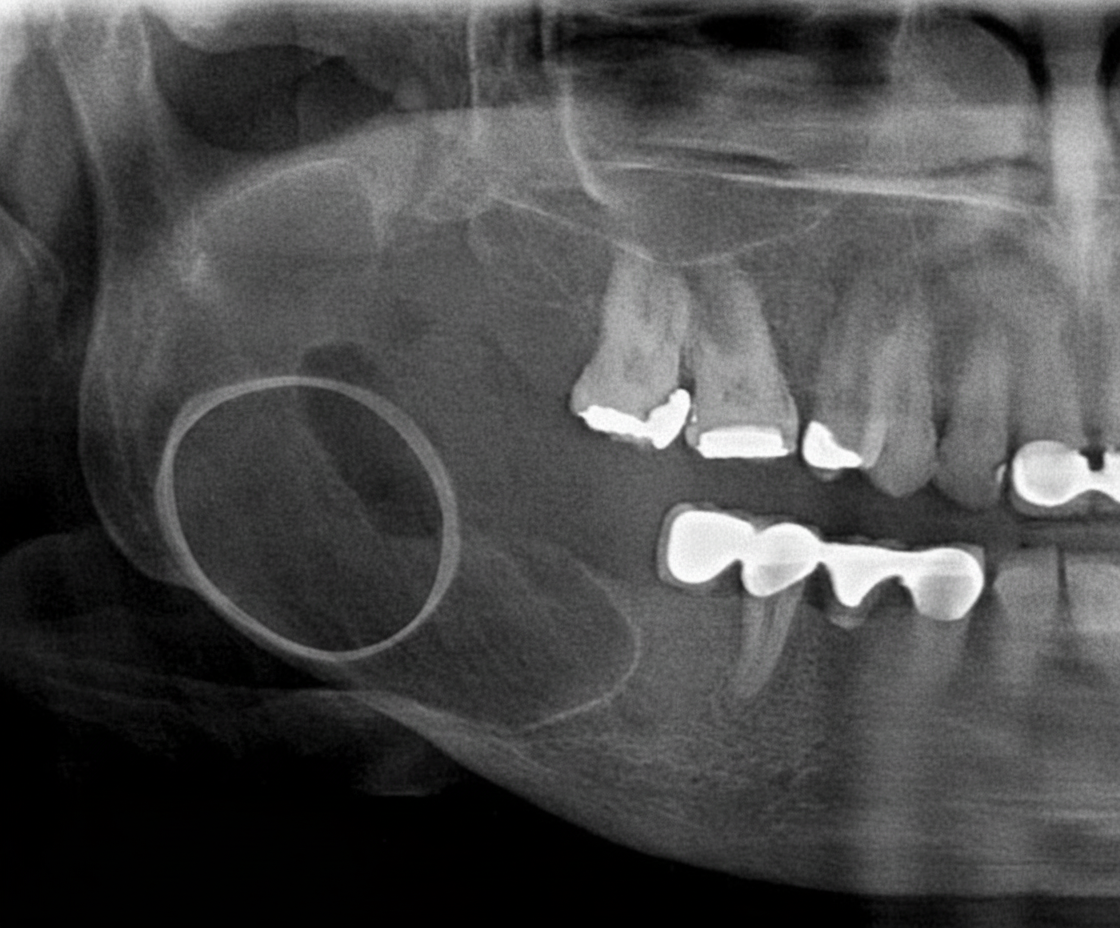
A radiograph of a 32-year-old patient reveals an asymptomatic lesion that was an accidental finding. What is the most likely diagnosis?
What is the best investigation to detect calcification?
A patient with a history of trauma presents with hearing loss. A High-Resolution Computed Tomography (HRCT) scan was performed. Which of the following structures is not typically visualized on HRCT?
Identify the rib highlighted in the X-ray.
In the given barium swallow image, which of the following shows the left atrium impression on the esophagus?
The structure marked by arrow in CT abdomen:

Practice by Chapter
Radiographic Anatomy of Skull and Face
Practice Questions
Radiographic Anatomy of Spine
Practice Questions
Radiographic Anatomy of Chest
Practice Questions
Radiographic Anatomy of Abdomen
Practice Questions
Radiographic Anatomy of Extremities
Practice Questions
Cross-sectional Anatomy: Brain and Head
Practice Questions
Cross-sectional Anatomy: Neck
Practice Questions
Cross-sectional Anatomy: Thorax
Practice Questions
Cross-sectional Anatomy: Abdomen and Pelvis
Practice Questions
Vascular Anatomy
Practice Questions
Developmental Anatomy Variations
Practice Questions
Anatomic Landmarks for Interventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app