
Radiological Anatomy — MCQs

On this page
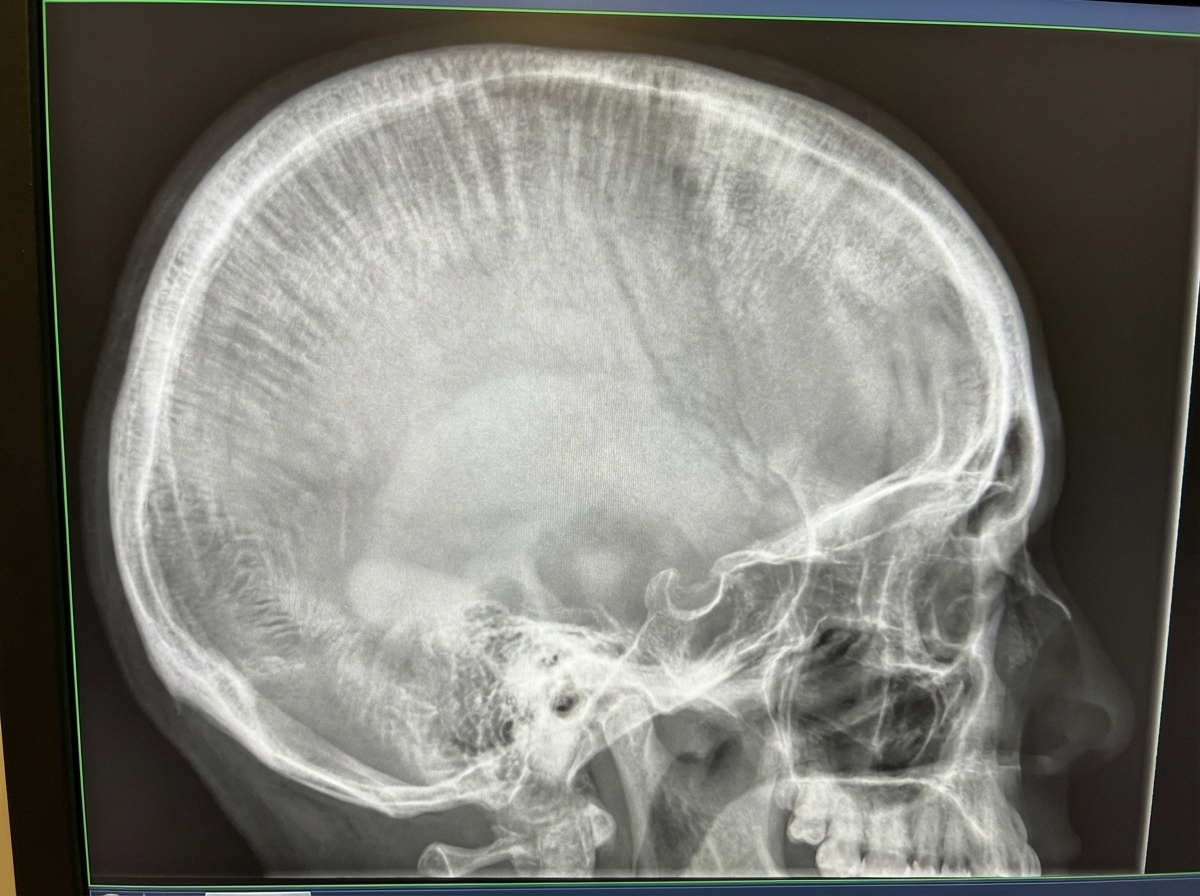
Which of the following conditions can manifest with the shown X-ray findings in the skull?
Which region in the crown of a tooth is often mistaken for caries in an intraoral periapical radiograph?
A 15-year-old male patient presents with pain in a lower back tooth and a history of frequent snacking. Intra-oral examination reveals occlusal caries on teeth 16 and 36, proximal caries between teeth 26 and 27, and a grossly carious tooth 46. Which of the following must be used when taking a radiograph for this patient?
Bitewing radiographs are best suited to monitor:
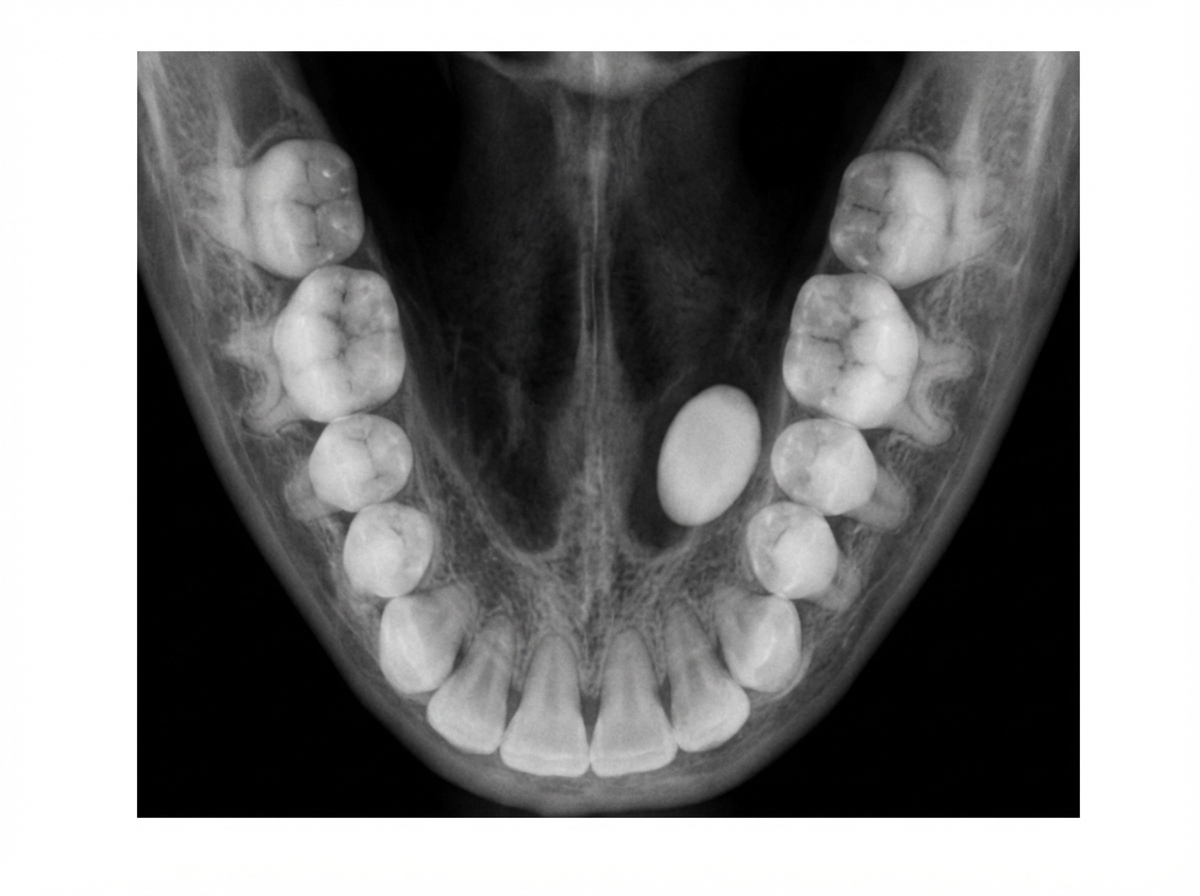
The following occlusal radiograph shows:
A 50-year-old male patient complains of reduced mouth opening. The patient has a history of a Road Traffic Accident (RTA) one week prior. A submentovertex view x-ray was taken which revealed a zygomatic arch fracture. Which of the following is true regarding the central beam in this x-ray?
Insal-Salvati index is used for evaluation of which bone?
Which bones ossify at birth?
Which of the following structures is not visualized on a coronal CT scan of the paranasal sinuses?
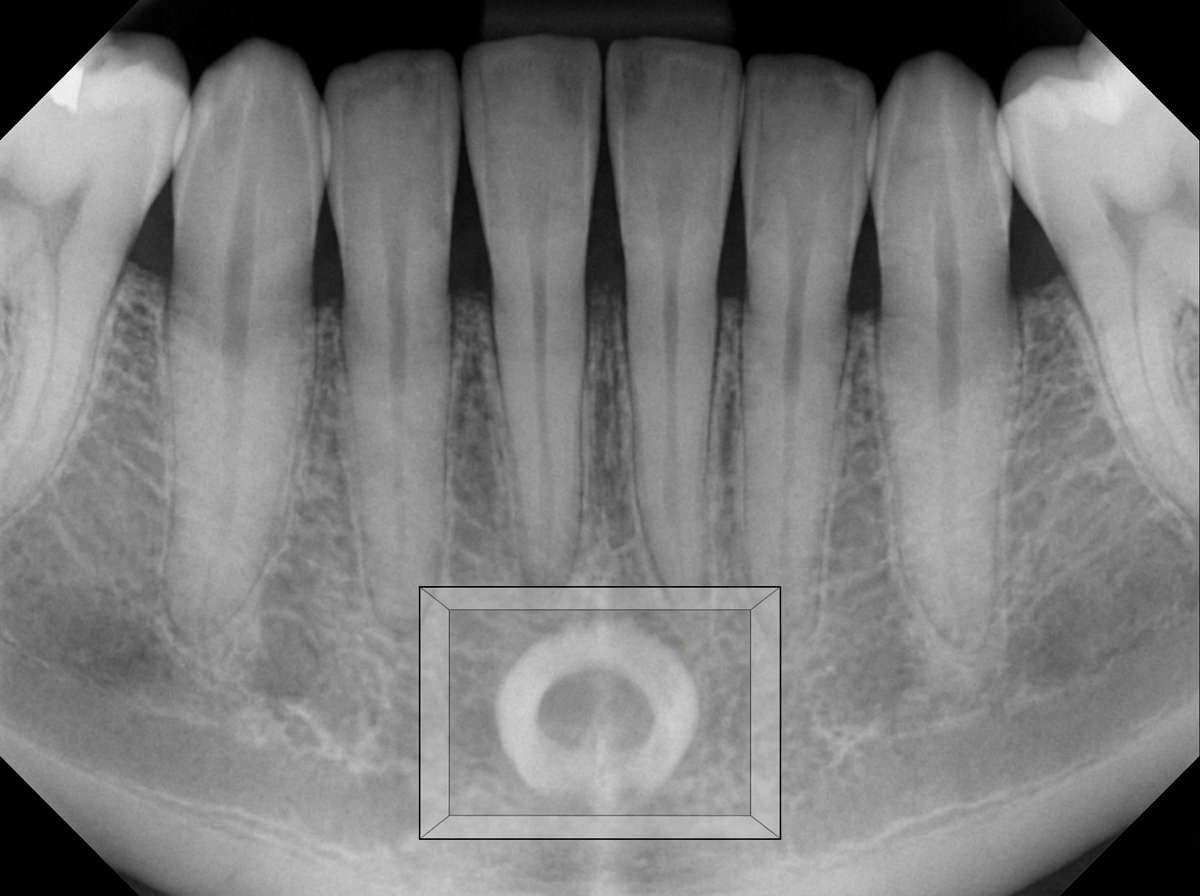
The radiopaque structure shown in the box is most likely:
Practice by Chapter
Radiographic Anatomy of Skull and Face
Practice Questions
Radiographic Anatomy of Spine
Practice Questions
Radiographic Anatomy of Chest
Practice Questions
Radiographic Anatomy of Abdomen
Practice Questions
Radiographic Anatomy of Extremities
Practice Questions
Cross-sectional Anatomy: Brain and Head
Practice Questions
Cross-sectional Anatomy: Neck
Practice Questions
Cross-sectional Anatomy: Thorax
Practice Questions
Cross-sectional Anatomy: Abdomen and Pelvis
Practice Questions
Vascular Anatomy
Practice Questions
Developmental Anatomy Variations
Practice Questions
Anatomic Landmarks for Interventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app