
Radiological Anatomy — MCQs

On this page
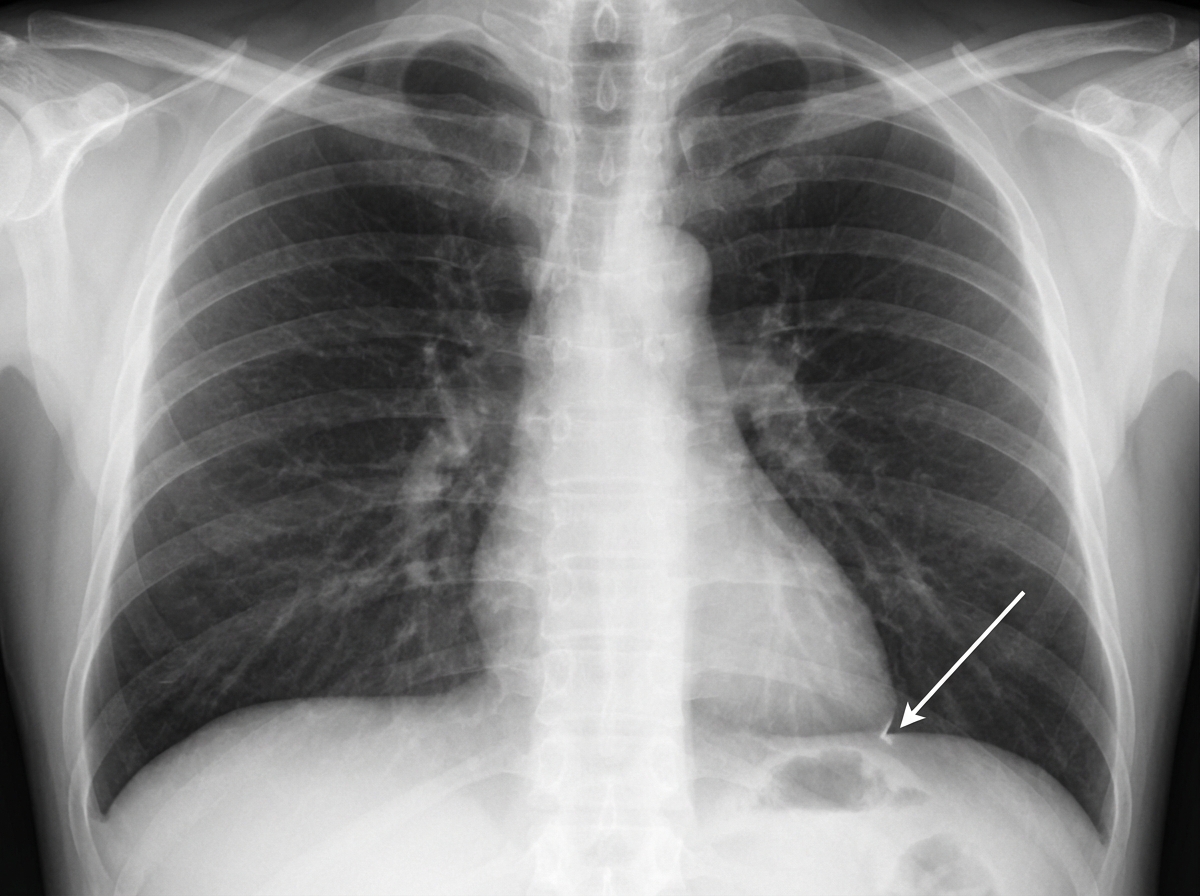
All of the following are true in a chest X-ray PA view EXCEPT:
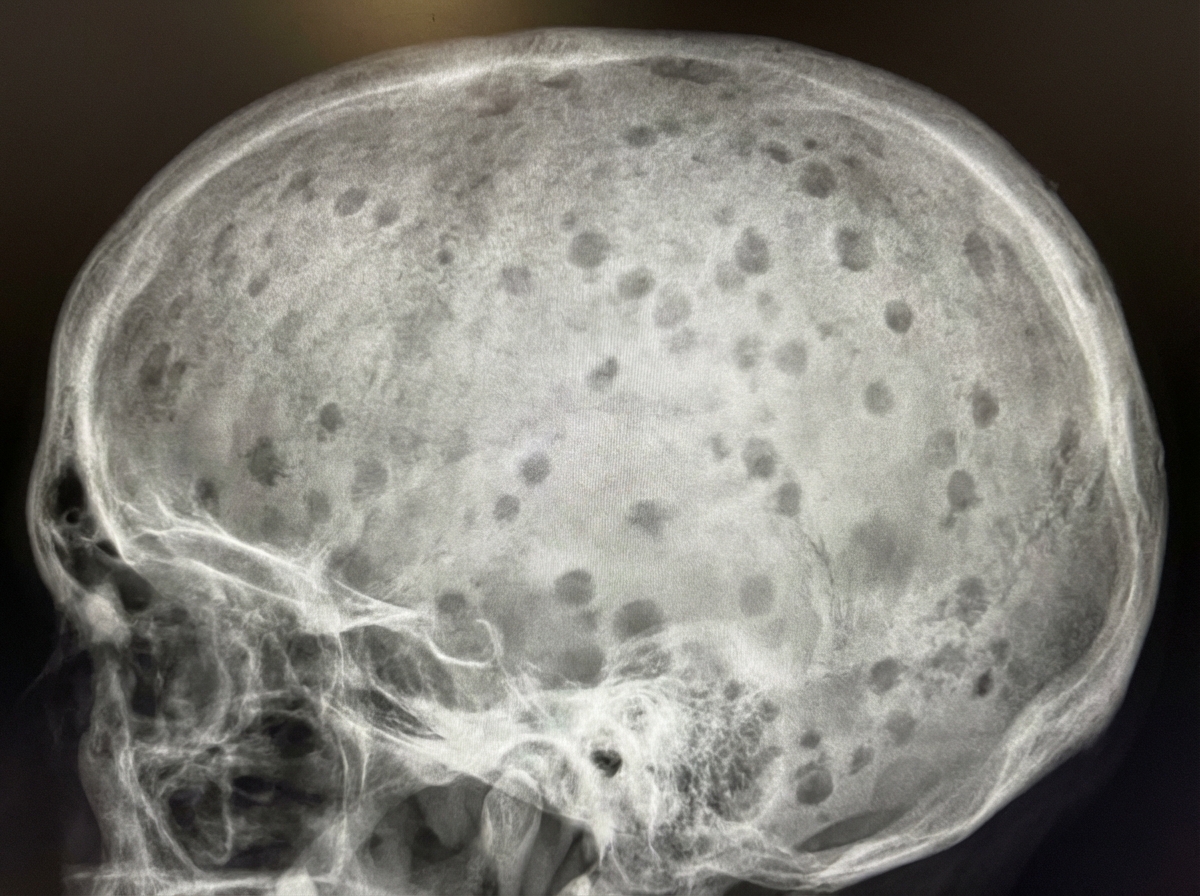
What is shown in the X-ray skull?
Identify the structure indicated in the given chest X-ray.
At 1 year of age, how many carpal bones are typically visible on a skiagram of the hand?
'Towne's view' in X-ray is used for visualizing which of the following structures?
The radiological feature of Pindborg's tumour is:
The 'hair on end' appearance on a skull X-ray is characteristic of which condition?
A low kilovoltage technique is most advantageous in demonstrating which of the following?
Shenton line is a radiological landmark seen in which joint on X-ray?
Wide diploic space of the skull with a brush border (hair on end) appearance is characteristic of which condition?
Practice by Chapter
Radiographic Anatomy of Skull and Face
Practice Questions
Radiographic Anatomy of Spine
Practice Questions
Radiographic Anatomy of Chest
Practice Questions
Radiographic Anatomy of Abdomen
Practice Questions
Radiographic Anatomy of Extremities
Practice Questions
Cross-sectional Anatomy: Brain and Head
Practice Questions
Cross-sectional Anatomy: Neck
Practice Questions
Cross-sectional Anatomy: Thorax
Practice Questions
Cross-sectional Anatomy: Abdomen and Pelvis
Practice Questions
Vascular Anatomy
Practice Questions
Developmental Anatomy Variations
Practice Questions
Anatomic Landmarks for Interventional Procedures
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app