
Shielding Design and Calculations — MCQs

All are done to minimize radiation exposure to the patient under fluoroscopy, except which of the following?
One gray equals
What is the recommended thickness of lead apron to prevent radiation exposure?
The substance most commonly used for protection against X-ray radiation is?
At t = 0 there are 6 x 10^23 radioactive atoms of a substance, which decay with a disintegration constant (λ) equal to 0.01/sec. What would be the initial decay rate?
Which of the following is the mechanism involved in X -ray production?
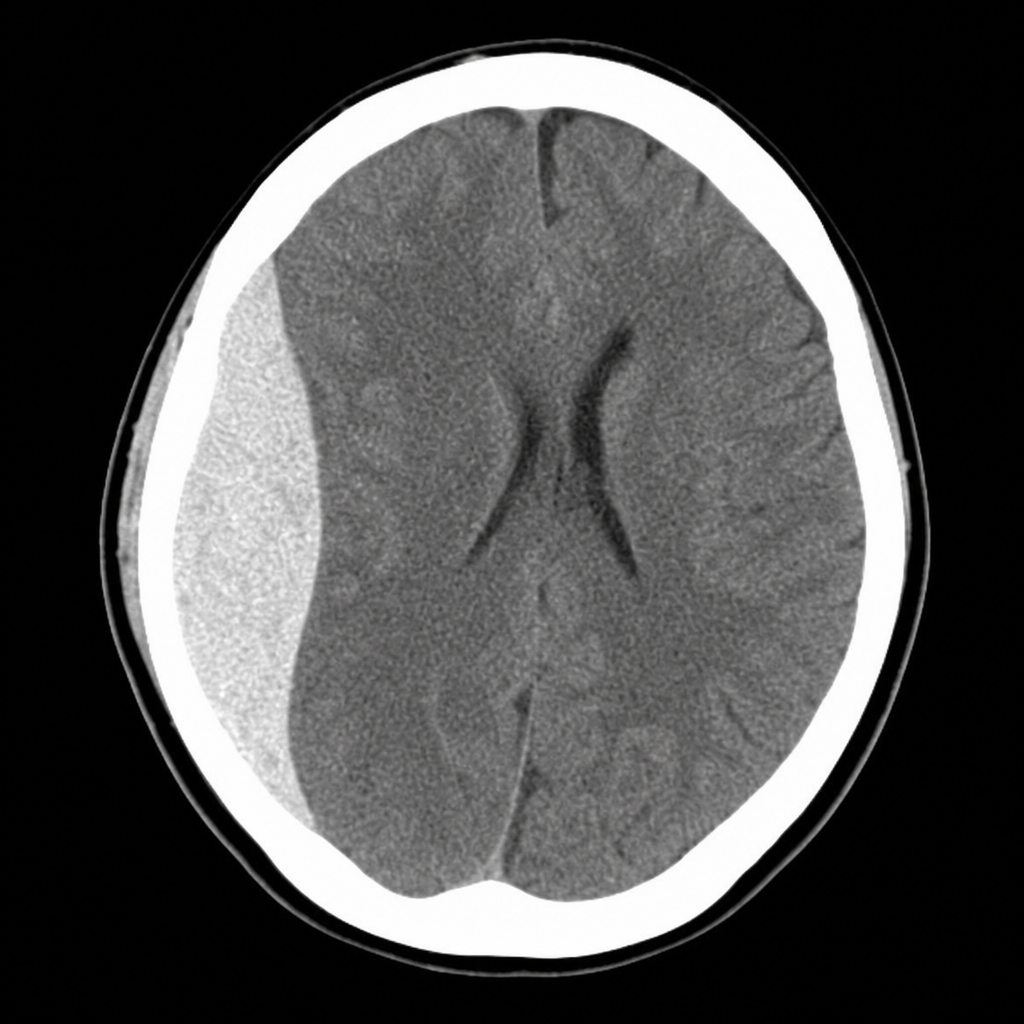
A 19-year-old male is brought to casualty after a road traffic accident. He had a brief loss of consciousness, followed by a lucid interval, and is now becoming increasingly drowsy with a GCS of 10. His right pupil is dilated and sluggishly reactive. The CT scan is shown in Image 1. Which vessel injury is most directly responsible for the collection seen?
Which of the following is the best method for radiation protection of the operator?
What is the primary function of a Bucky diaphragm?
What is the result of using filters in diagnostic radiology beams?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app