
Radiation Physics and Protection — MCQs

On this page
Regarding CT scan, all of the following are true EXCEPT?
What is used to prevent radiation exposure in an operation theatre?
Collimating the X-ray beam reduces the formation of scattered radiation by?
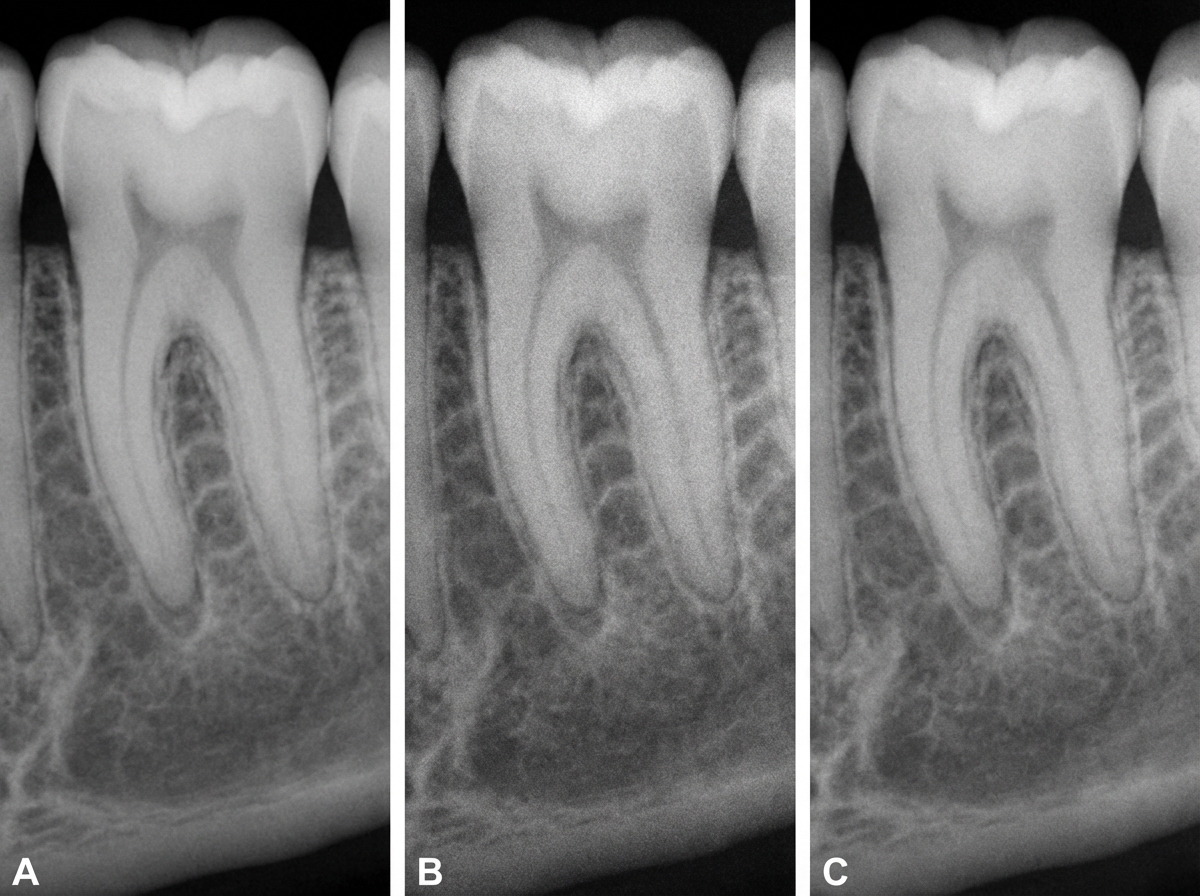
Three radiographs of the same tooth were taken using a digital intra-oral X-ray system, an intensifying screen/film cassette combination, and conventional dental film (F speed). Which of the following X-rays was taken with conventional dental film?
Which of the following is hypointense (dark) on T2-weighted MRI?
The 10-day rule is related to which of the following?
Radio frequency waves are used in which of the following imaging modalities?
CT or Hounsfield numbers depend upon:
A 45-year-old male presents with pain in the right upper back region. On intraoral examination, carious tooth 16 is noted. The clinician decides to use the long cone technique for taking a radiograph. What is the primary benefit of using this technique?
Which of the following has the greatest penetration power?
Practice by Chapter
Electromagnetic Radiation
Practice Questions
X-ray Production
Practice Questions
Interaction of Radiation with Matter
Practice Questions
Radiation Measurement Units
Practice Questions
Radiation Detectors
Practice Questions
Radiobiology Fundamentals
Practice Questions
Radiation Protection Principles
Practice Questions
Personnel Monitoring
Practice Questions
Shielding Design and Calculations
Practice Questions
Radiation Dose Optimization
Practice Questions
Regulatory Requirements
Practice Questions
Radiation Accidents Management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app