
Radiation Physics and Protection — MCQs

On this page
What is the ICRP recommended genetic dose of radiation exposure for the general population?
Which imaging modality involves the least radiation exposure?
What is the SI unit of dose equivalent of radiation?
On taking an X-ray, where is the grid placed?
Which of the following isotopes has the longest half-life?
Which material is commonly used for X-ray exposure prevention screens?
Which of the following is NOT mutagenic?
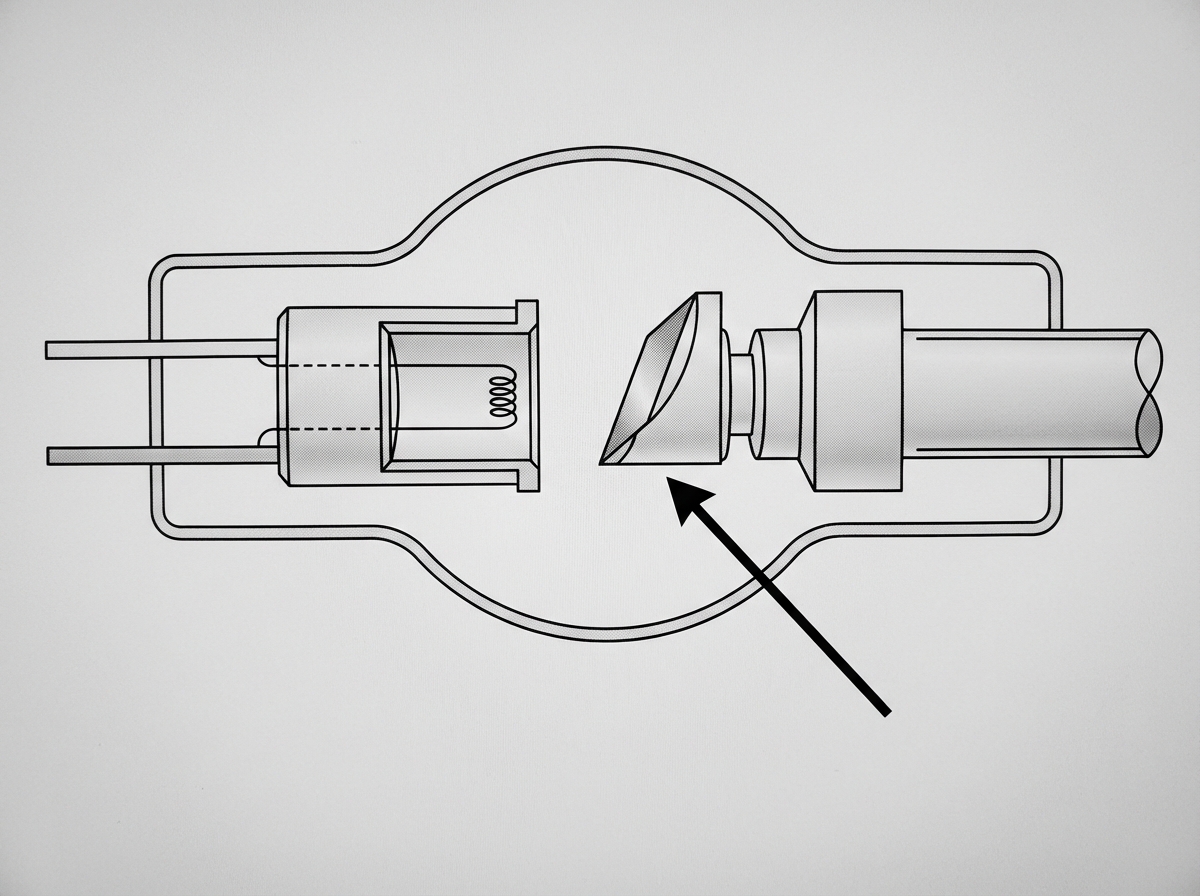
Identify the component indicated by the arrow.
An airline flight of 5 hours in the middle latitudes at an altitude of 12 km may result in an exposure of _____ µSv.
What type of particle does Phosphorus-32 emit?
Practice by Chapter
Electromagnetic Radiation
Practice Questions
X-ray Production
Practice Questions
Interaction of Radiation with Matter
Practice Questions
Radiation Measurement Units
Practice Questions
Radiation Detectors
Practice Questions
Radiobiology Fundamentals
Practice Questions
Radiation Protection Principles
Practice Questions
Personnel Monitoring
Practice Questions
Shielding Design and Calculations
Practice Questions
Radiation Dose Optimization
Practice Questions
Regulatory Requirements
Practice Questions
Radiation Accidents Management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app