
Radiation Physics and Protection — MCQs

On this page
Which of the following is the mechanism involved in X -ray production?
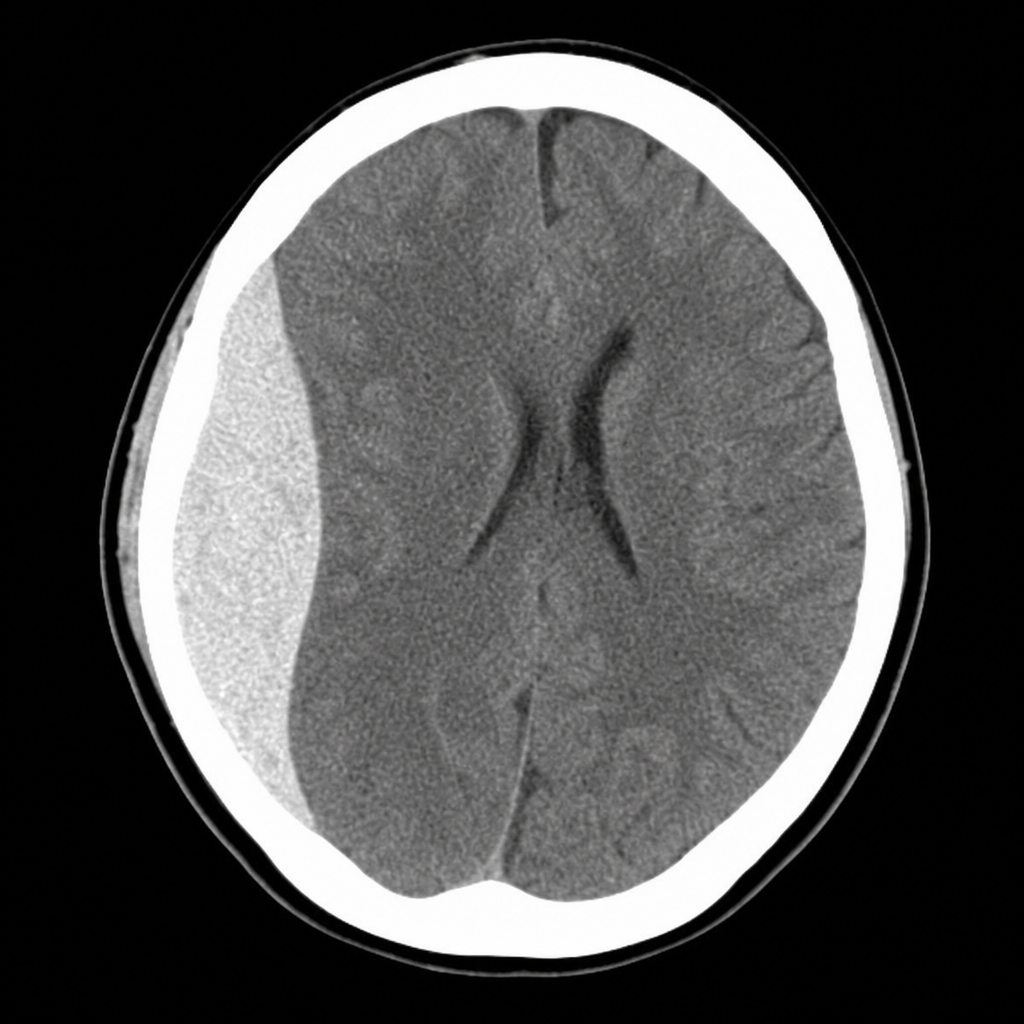
A 19-year-old male is brought to casualty after a road traffic accident. He had a brief loss of consciousness, followed by a lucid interval, and is now becoming increasingly drowsy with a GCS of 10. His right pupil is dilated and sluggishly reactive. The CT scan is shown in Image 1. Which vessel injury is most directly responsible for the collection seen?
Which of the following is the best method for radiation protection of the operator?
What is the primary function of a Bucky diaphragm?
What is the result of using filters in diagnostic radiology beams?
For normal mammography, what is the nominal focal size of the X-ray tube used?
What type of magnet is used in MRI?
Which X-rays are most likely to be absorbed by tissues and produce injury?
The 'heel effect' results in what kind of X-ray beam intensity distribution?
Which statement is true regarding CT dose index?
Practice by Chapter
Electromagnetic Radiation
Practice Questions
X-ray Production
Practice Questions
Interaction of Radiation with Matter
Practice Questions
Radiation Measurement Units
Practice Questions
Radiation Detectors
Practice Questions
Radiobiology Fundamentals
Practice Questions
Radiation Protection Principles
Practice Questions
Personnel Monitoring
Practice Questions
Shielding Design and Calculations
Practice Questions
Radiation Dose Optimization
Practice Questions
Regulatory Requirements
Practice Questions
Radiation Accidents Management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app