
Pediatric Radiology — MCQs

On this page
Excretory urogram in a two-year-old child with recurrent UTI shows what named radiographic sign?

An 11-month-old child presents with recurrent episodes of UTI. MCUG shows VUR:

The given radiograph is diagnostic of:

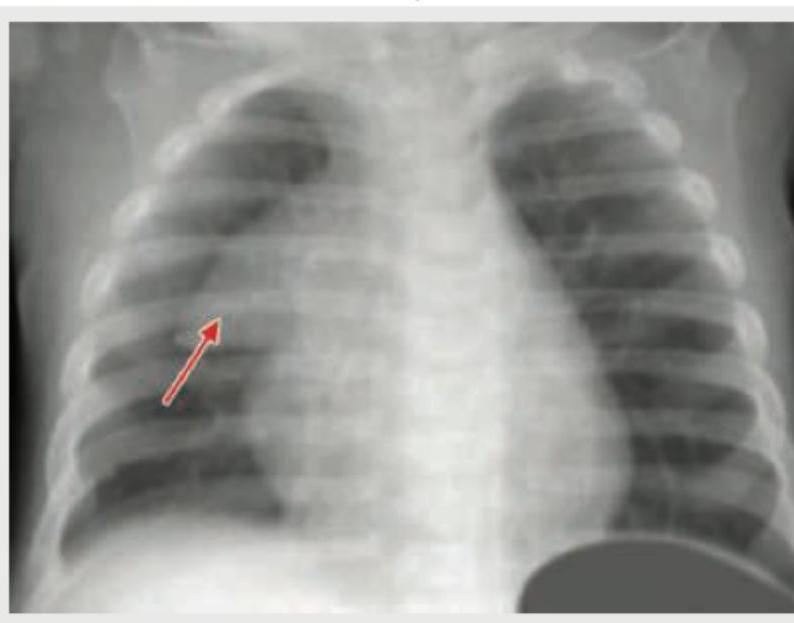
Comment on the arrow marked structure in CXR of an infant: (Recent NEET Pattern 2018-19)
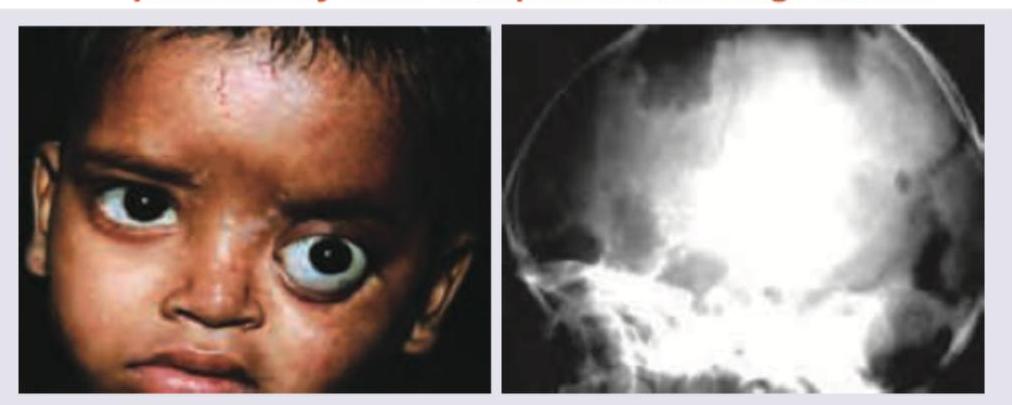
A child presents with the following appearance, seborrheic dermatitis, hepatosplenomegaly, and pancytopenia. X-ray of the skull is shown. What skull radiographic appearance is shown?
A "double bubble" sign on an antenatal ultrasound examination in a gravid woman is diagnostic of
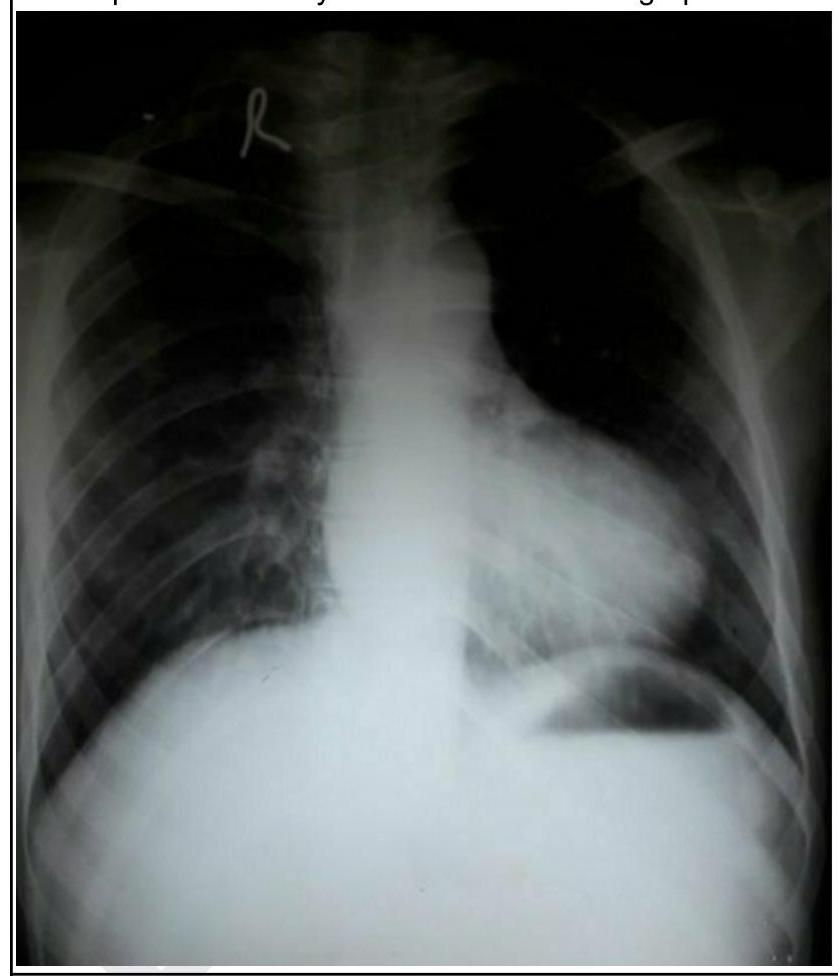
A child presents with cyanosis. His chest radiograph is shown below. What is the diagnosis?
What condition is associated with the sign seen in the given USG?

Investigation of choice for Posterior urethral valves?
The most likely diagnosis in a newborn who had a radiopaque shadow with an air-fluid level in the chest along with hemivertebrae of the 6th thoracic vertebra on plain X-ray is –
Practice by Chapter
Normal Pediatric Developmental Anatomy
Practice Questions
Neonatal Imaging
Practice Questions
Pediatric Chest Imaging
Practice Questions
Pediatric Abdominal Imaging
Practice Questions
Pediatric Musculoskeletal Imaging
Practice Questions
Pediatric Neuroradiology
Practice Questions
Congenital Heart Disease Imaging
Practice Questions
Pediatric Oncology Imaging
Practice Questions
Child Abuse Imaging
Practice Questions
Pediatric Interventional Radiology
Practice Questions
Radiation Protection in Pediatrics
Practice Questions
Sedation in Pediatric Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app