
Pediatric Radiology — MCQs

On this page
Which contrast material is used in the diagnosis of esophageal atresia?
The time usually taken for air to reach the descending colon after birth in a normal infant is:
The provided X-ray image depicts which of the following conditions?

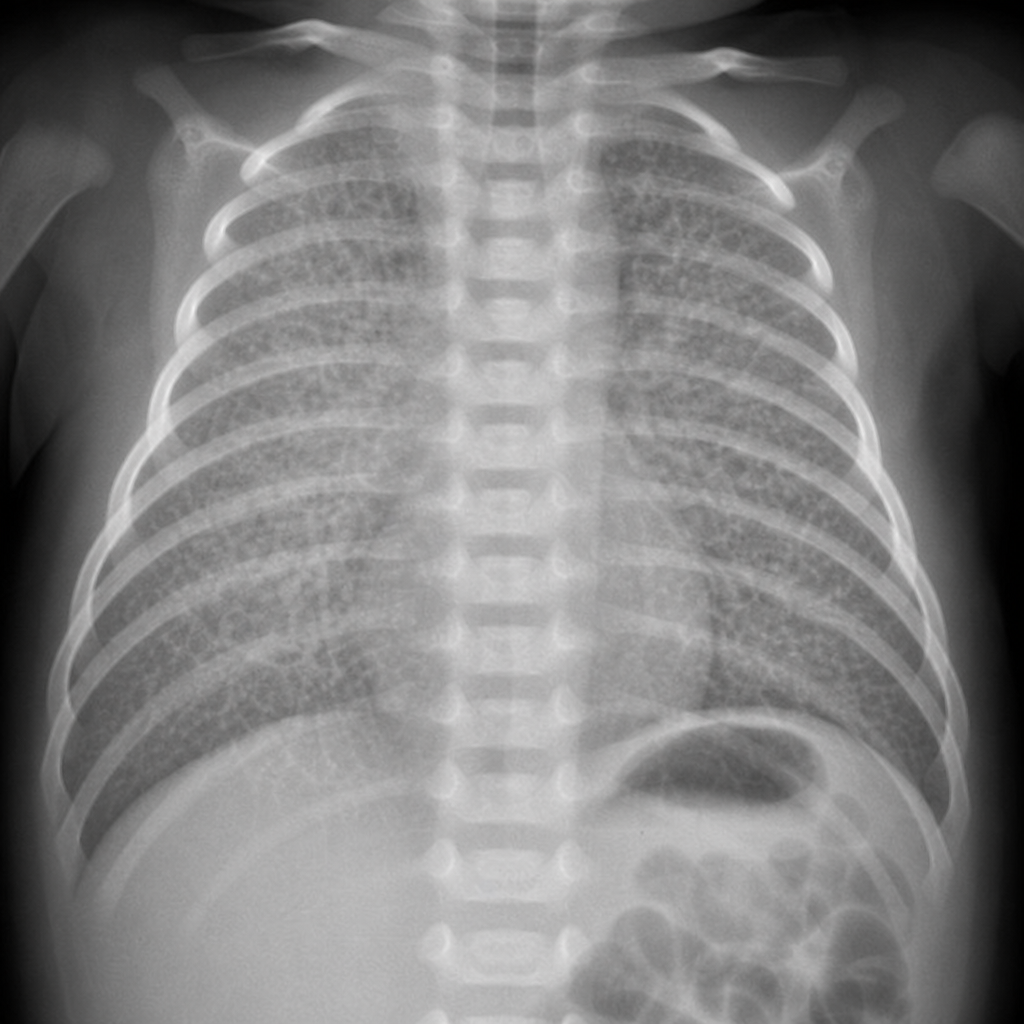
A chest radiograph from a premature infant with respiratory distress beginning shortly after birth is provided. What is the probable diagnosis?
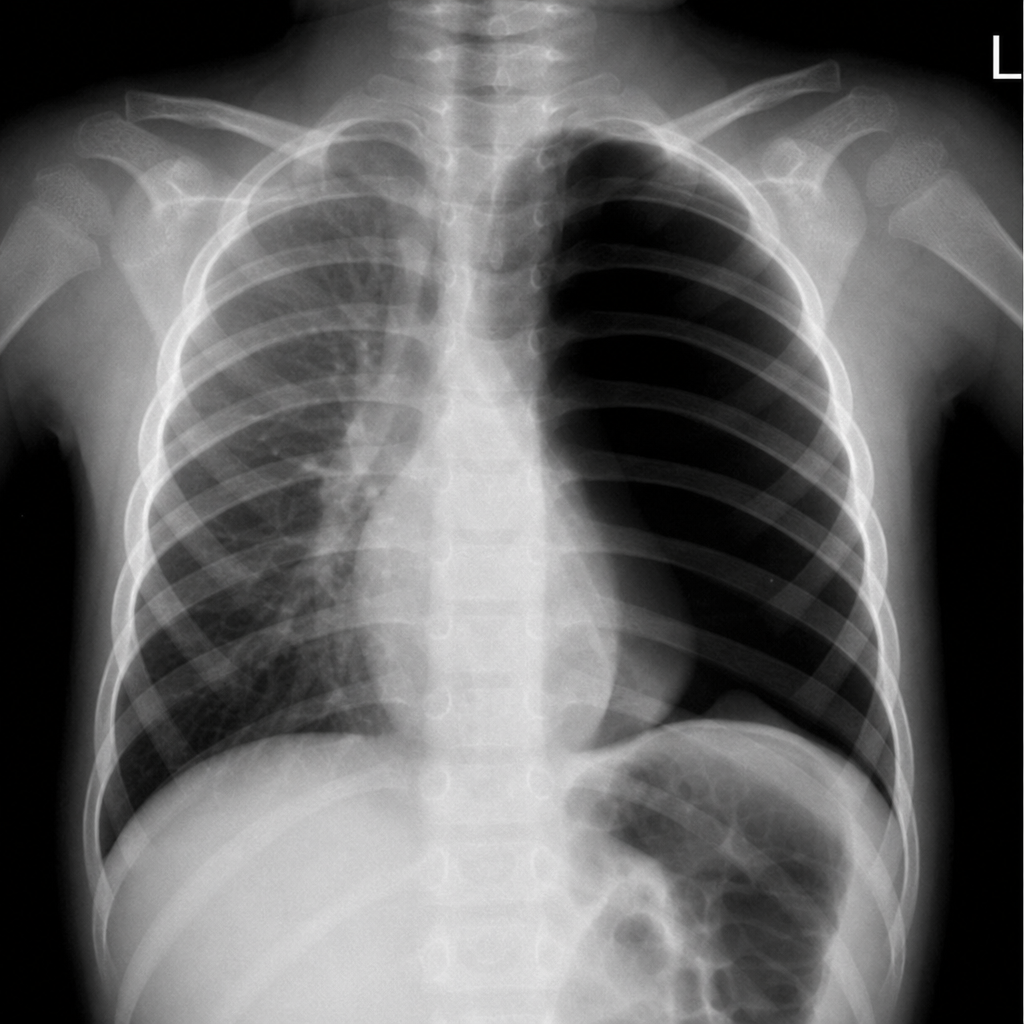
What is the most likely diagnosis based on a chest x-ray of a child presenting with acute breathlessness?
Scrotal calcifications in fetal sonography may be seen in which of the following conditions?
Which one of the following is the earliest radiographic manifestation of childhood leukemia?
What is the investigation of choice for hydrocephalus in infants?
Intra-abdominal calcification in a plain X-ray of the abdomen is most often seen in which of the following conditions?
"Double bubble" sign is a feature of which of the following conditions?
Practice by Chapter
Normal Pediatric Developmental Anatomy
Practice Questions
Neonatal Imaging
Practice Questions
Pediatric Chest Imaging
Practice Questions
Pediatric Abdominal Imaging
Practice Questions
Pediatric Musculoskeletal Imaging
Practice Questions
Pediatric Neuroradiology
Practice Questions
Congenital Heart Disease Imaging
Practice Questions
Pediatric Oncology Imaging
Practice Questions
Child Abuse Imaging
Practice Questions
Pediatric Interventional Radiology
Practice Questions
Radiation Protection in Pediatrics
Practice Questions
Sedation in Pediatric Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app