
Pediatric Radiology — MCQs

On this page
Which of the following is NOT a radiological feature of ileal atresia?
Which of the following signs is associated with CHPS?
Which of the following is NOT an X-ray finding of retinoblastoma?
What is the initial imaging of choice for suspected acute appendicitis in children?
Snow storm ascites is seen in which of the following conditions?
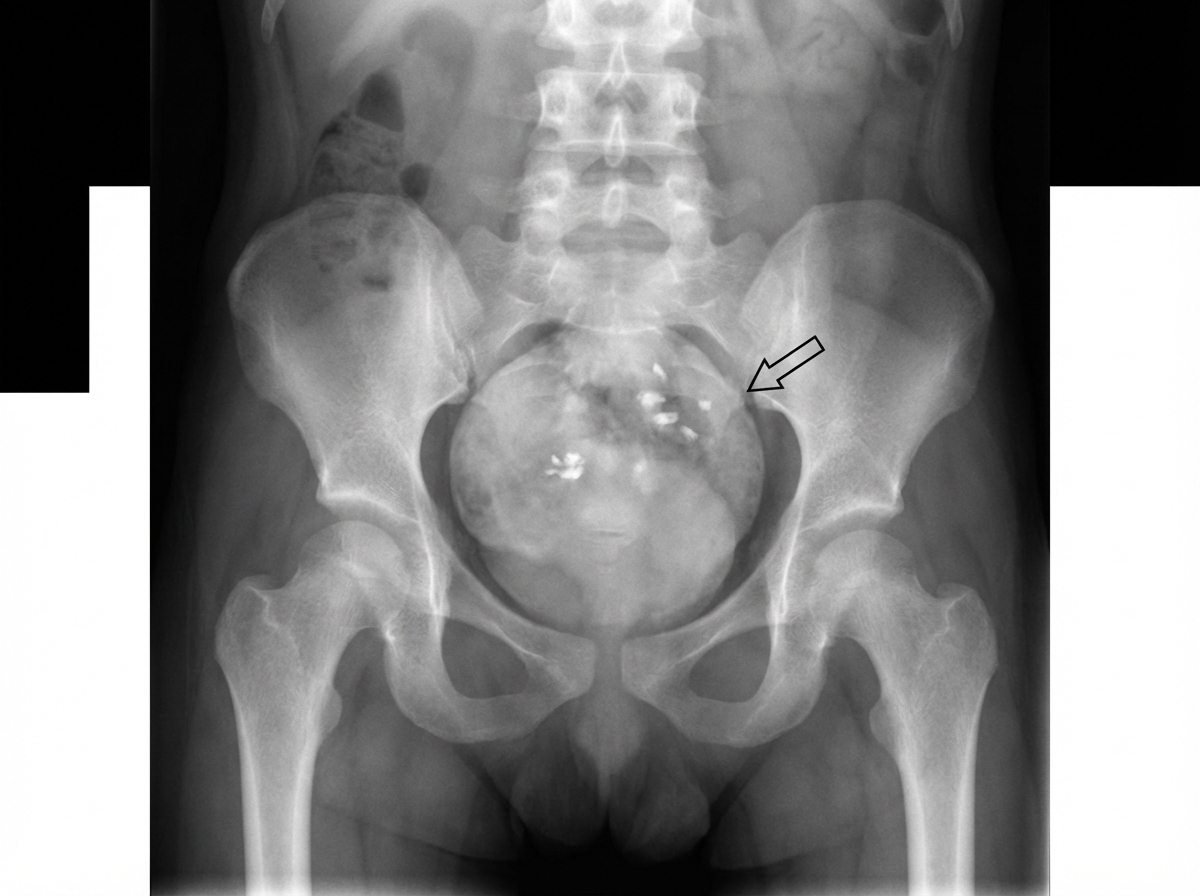
Which condition is shown in the image?

What is the maximum limit of the cardiothoracic ratio in children below 2 years of age?
A patient admitted with an abdominal mass underwent MRI, which revealed bilateral adrenal calcification. What is the most likely diagnosis?
An infantogram shows the presence of which of the following?
What is the first sign of hydrocephalus in children?
Practice by Chapter
Normal Pediatric Developmental Anatomy
Practice Questions
Neonatal Imaging
Practice Questions
Pediatric Chest Imaging
Practice Questions
Pediatric Abdominal Imaging
Practice Questions
Pediatric Musculoskeletal Imaging
Practice Questions
Pediatric Neuroradiology
Practice Questions
Congenital Heart Disease Imaging
Practice Questions
Pediatric Oncology Imaging
Practice Questions
Child Abuse Imaging
Practice Questions
Pediatric Interventional Radiology
Practice Questions
Radiation Protection in Pediatrics
Practice Questions
Sedation in Pediatric Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app