
Pediatric Radiology — MCQs

On this page
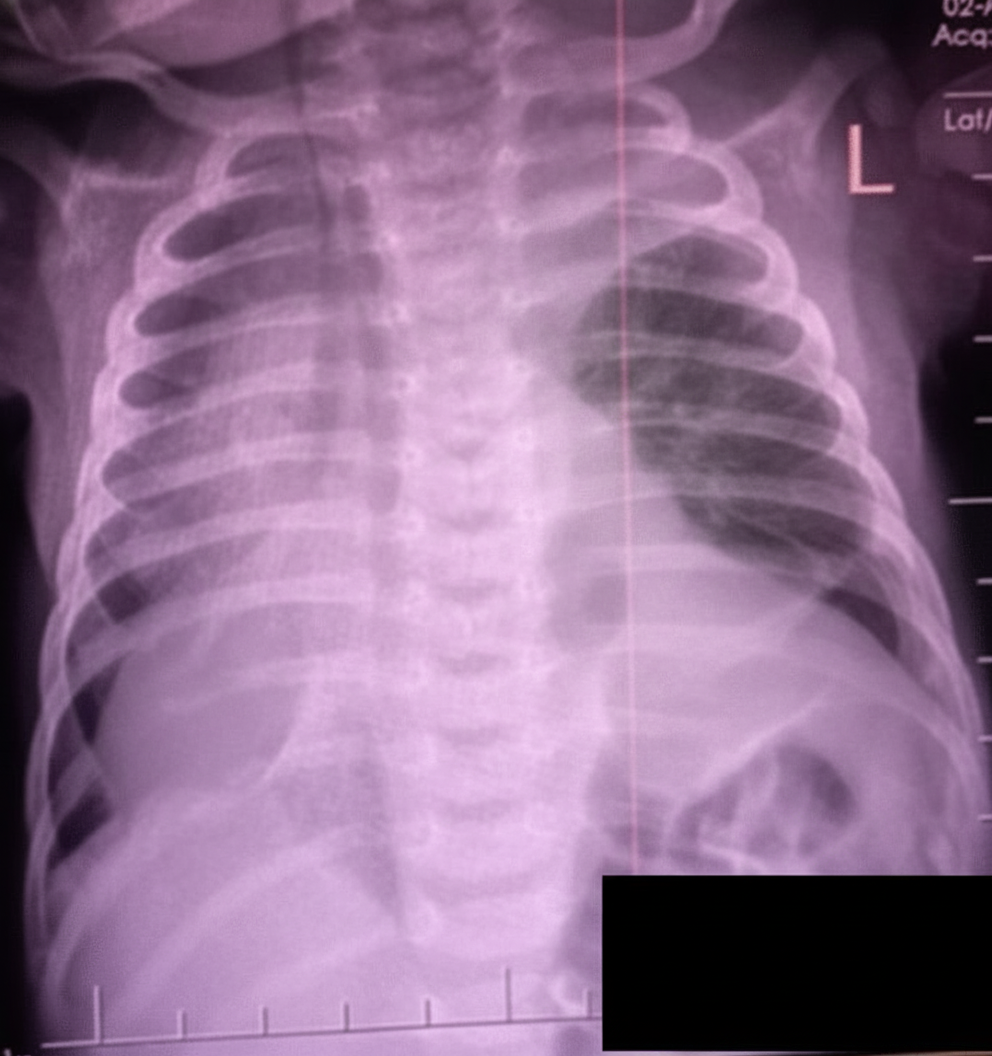
A 3-day-old child presents with the below CXR. What is the diagnosis?
What is the initial imaging of choice for intussusception?
What is the investigation of choice for studying vesico-ureteric reflux?
Gasless abdomen on X-ray is found in all except:
The diagnostic feature of congenital diaphragmatic hernia on prenatal ultrasonography is:
Neuroblastoma differs from Wilm's tumor radiologically by all EXCEPT?
The double bubble sign is typically seen in which of the following conditions?
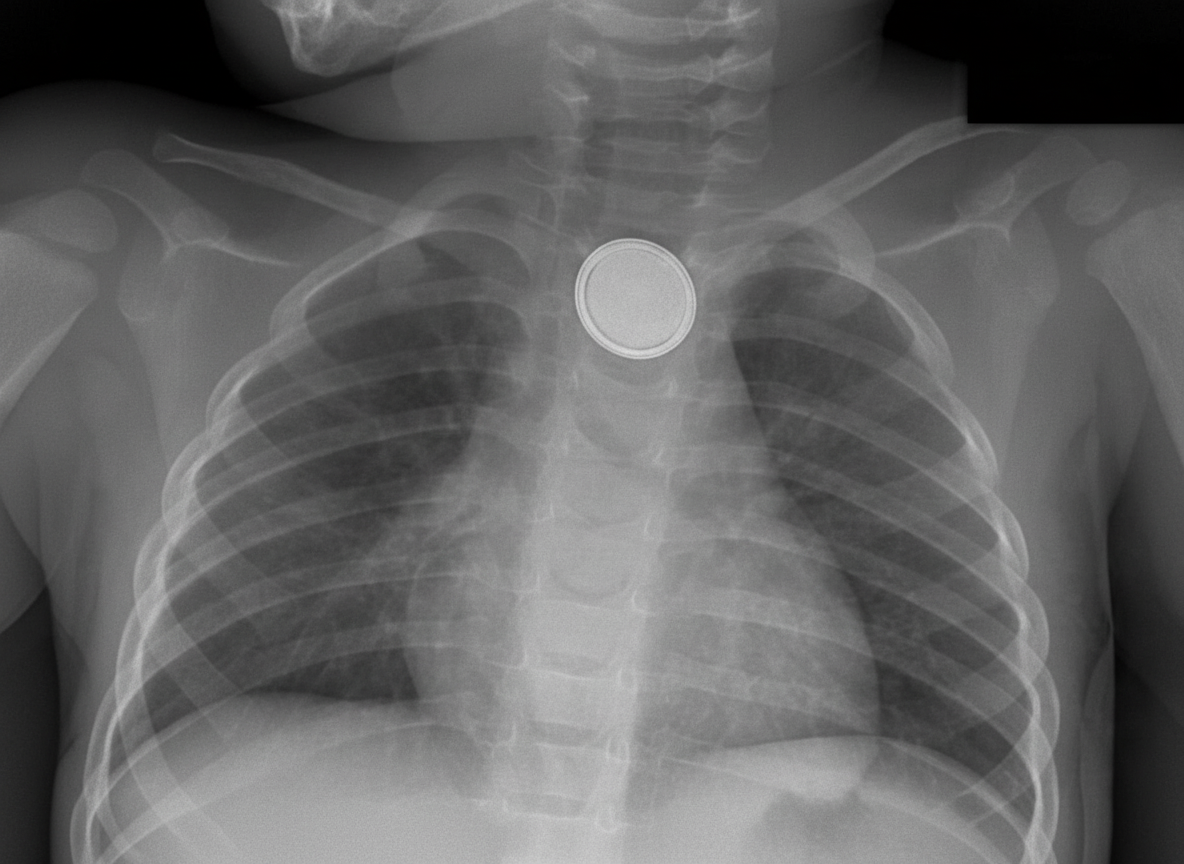
A 4-year-old child presents with findings on a chest X-ray. What is the probable location of the foreign body visible on the skiagram?
The 'keyhole sign' is a radiological finding typically associated with which of the following conditions?
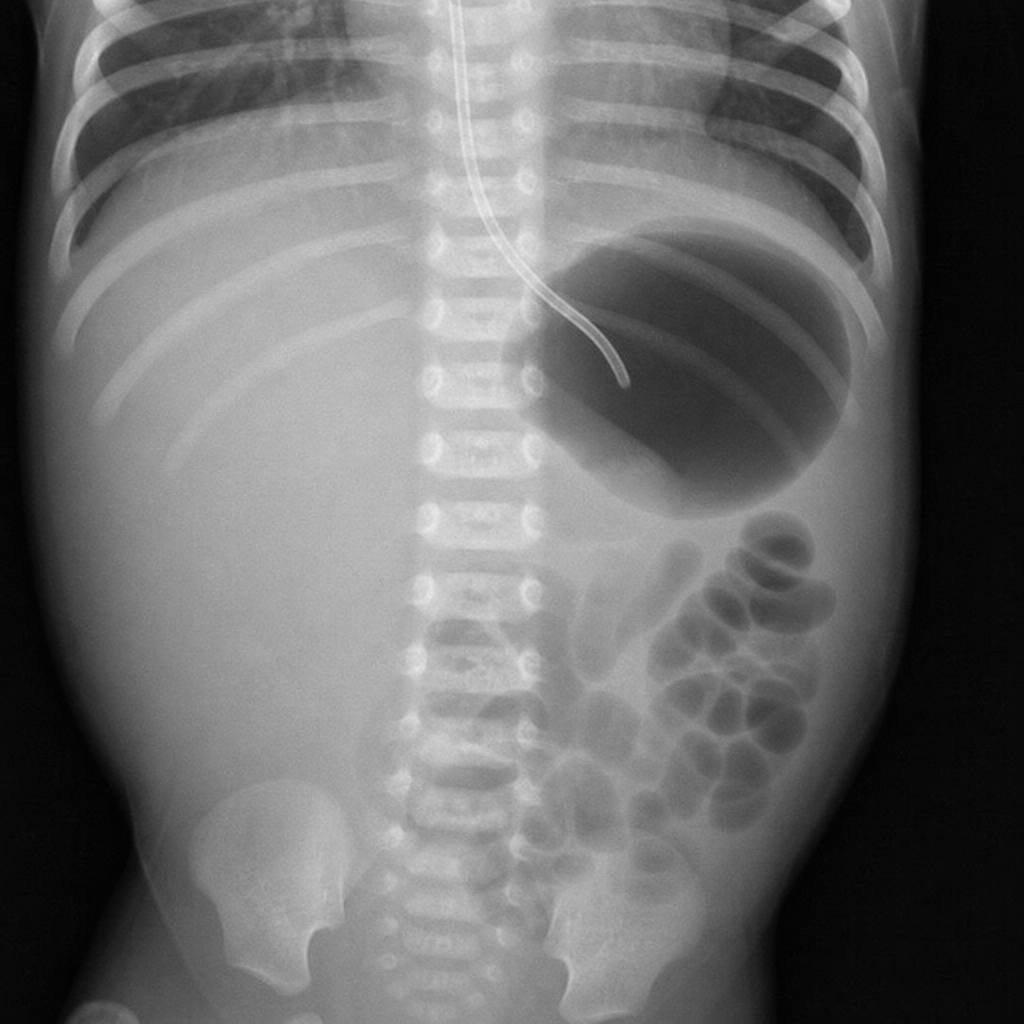
Interpret the plain X-ray of the abdomen:
Practice by Chapter
Normal Pediatric Developmental Anatomy
Practice Questions
Neonatal Imaging
Practice Questions
Pediatric Chest Imaging
Practice Questions
Pediatric Abdominal Imaging
Practice Questions
Pediatric Musculoskeletal Imaging
Practice Questions
Pediatric Neuroradiology
Practice Questions
Congenital Heart Disease Imaging
Practice Questions
Pediatric Oncology Imaging
Practice Questions
Child Abuse Imaging
Practice Questions
Pediatric Interventional Radiology
Practice Questions
Radiation Protection in Pediatrics
Practice Questions
Sedation in Pediatric Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app